Standardized Screening for Health-Related Social Needs in Clinical Settings: The Accountable Health Communities Screening Tool
The impacts of unmet health-related social needs, such as homelessness, inconsistent access to food, and exposure to violence on health and health care utilization, are well-established. Growing evidence indicates that addressing these and other needs can help reverse their damaging health effects, but screening for social needs is not yet standard clinical practice. In many communities, the absence of established pathways and infrastructure and perceptions of inadequate time to make community referrals are barriers that seem to often keep clinicians and their staff from broaching the topic. The Centers for Medicare & Medicaid Services (CMS) Accountable Health Communities Model, tested by the Center for Medicare and Medicaid Innovation, addresses this critical gap between clinical care and community services in the current health care delivery system by testing whether systematically identifying and addressing the health-related social needs of Medicare and Medicaid beneficiaries impacts their total health care costs and improves health.
With input from a panel of national experts and after review of existing screening instruments, CMS developed a 10-item screening tool to identify patient needs in 5 different domains that can be addressed through community services (housing instability, food insecurity, transportation difficulties, utility assistance needs, and interpersonal safety). Clinicians and their staff can use this short tool across a spectrum of ages, backgrounds, and settings, and it is streamlined enough to be incorporated into busy clinical workflows. Just like with clinical assessment tools, results from this screening tool can be used to inform a patient’s treatment plan as well as make referrals to community services.
Introduction
Evidence demonstrates that non-medical health-related social needs (HRSNs), such as housing instability, food insecurity, and exposure to interpersonal violence, drive health care utilization and impact health outcomes [1, 2, 3]. Clinicians routinely employ standardized questions and validated assessment tools to screen for clinical and behavioral drivers of poor health, such as alcohol dependency, decompensated heart failure, and depression, but screening for HRSNs is not yet standard clinical practice [4, 5, 6]. Standardized application of screening tools as a part of clinical routines allows provider teams to quickly and consistently identify possible health needs for further investigation and intervention. A variety of assessment tools have been developed to help health providers identify the presence of deleterious social circumstances, and a few recent studies have demonstrated the efficacy of screening tools combining several HRSN domains in identifying various HRSNs of patients and their caregivers [7, 8, 9]. However, inadequate training, perceptions of inadequate time to investigate social needs, and, importantly, the absence of established pathways and infrastructure to address identified unmet needs are barriers that often keep clinicians and their staff from implementing HRSN screening at their clinical delivery sites [10, 11, 12]. The Centers for Medicare & Medicaid Services (CMS) Accountable Health Communities (AHC) Model will test whether addressing these delivery system barriers through universal HRSN screening and enhanced clinical-community linkages can improve health outcomes and impact costs [13].
CMS developed the AHC Model to address a critical gap between clinical care and community services in the current health care delivery system by testing whether systematically identifying and addressing the HRSNs of Medicare and Medicaid beneficiaries impacts total health care costs and utilization, increases the quality of care, and improves health. Through the model, CMS will support clinical and community partnerships—coordinated by a “backbone” organization—among clinical delivery sites, community service providers, and state Medicaid agencies. Clinical delivery sites—hospitals, clinics, doctors’ offices, and other clinical settings—will serve as the crucial entry point for the model by serving as the place of screening for all Medicare and Medicaid beneficiaries for unmet needs across five core HRSN domains: housing instability (e.g., homelessness, poor housing quality), food insecurity, transportation difficulties, utility assistance needs, and interpersonal safety concerns (e.g., intimate-partner violence, elder abuse, child maltreatment). Individual communities may also elect to screen across several supplemental HRSN domains, including family and social supports (e.g., respite and caregiver support services, child care, social isolation), education, employment and financial strain, health behaviors (e.g., tobacco use, alcohol and substance use, physical activity), mental health, and disabilities. To ensure consistency in the screening offered to beneficiaries across both an individual community’s clinical delivery sites and across all the communities in the model, CMS developed a standardized HRSN screening tool. This paper describes the considerations and processes that shaped the screening tool, including the component questions and evidence supporting their inclusion, as well as the potential role the tool can play in facilitating screening for HRSNs in clinical settings across the U.S. health care system.
Tool Development: Design Principles and Expert Consultation
Out of the many non-medical needs that impact health, CMS selected five core HRSN domains based on the following criteria: 1) high-quality evidence exists linking the HRSN to poor health or increased health care utilization and cost; 2) the need can be met by community service providers; and 3) the need is not systemically addressed by health care providers. In developing the AHC HRSN screening tool for the five core domains, CMS followed three guiding principles.
First, the tool needed to consistently identify the broadest set of HRSNs that could be addressed by community service providers. Ideally, the screening tool would identify any unmet need within an inclusive focal area likely to have a negative impact on health, rather than specifying a particular subset of needs. The tool would allow clinical delivery sites to identify broad needs and engage navigators and community service providers, who are better suited to identify more specific needs and address the individualized issues that underlie unmet need. For example, the AHC HRSN screening tool would identify that an individual is at risk for food insecurity broadly, and the care navigator or community service provider would identify the individual’s specific drivers of food insecurity, such as difficulty obtaining food near the end of pay periods or daily need for food assistance.
Second, the tool needed to be simple and streamlined to ensure that its questions were readily understandable to the broadest audience across a variety of settings, as well as to allow for inclusion of routine screening in busy clinical workflows [14]. Medicare and Medicaid beneficiaries represent a diverse subset of the U.S. population and include individuals of all ages and backgrounds, and AHCs will span rural and urban areas across the United States. AHCs will work to make the tool accessible to beneficiaries regardless of language, literacy level or disability status, further broadening its applicability. Additionally, because AHC clinical delivery sites have the option to allow beneficiaries to self-administer the screening tool, simplicity in design and language were key considerations in order to reduce the need for outside assistance.
Finally, the tool needed to be evidence-based and informed by practical experience. CMS began by conducting a review of existing screening tools and questions focused on the core and supplemental HRSN domains listed above. Through this process, over 50 screening tools totaling more than 200 questions were compiled. In order to refine this list, CMS consulted a technical expert panel (TEP) consisting of a diverse group of tool developers, public health and clinical researchers, clinicians, population health and health systems executives, community-based organization leaders, and federal partners (Box 2). Over the course of several meetings, this TEP came together to discuss opportunities and challenges involved in screening for HRSNs; consider and pare down CMS’s list of evidence-based screening questions; and recommend a short list of questions for inclusion in the final tool.
The AHC Health-Related Social Needs Screening Tool
Based on the recommendations of the TEP, CMS developed a 10-question screening tool (the AHC HRSN screening tool) to identify unmet needs across five core domains. Questions in the AHC screening tool are meant for an individual respondent and should be answered by individuals themselves, or by a parent or caregiver on an individual’s behalf. The tool is designed to be short, accessible, consistent, and inclusive. The full AHC HRSN screening tool for use in the AHC Model will also include questions to identify a beneficiary’s eligibility for the model, standard demographic questions for evaluation purposes, and screening questions for supplemental domains, if applicable. Development of these sections is not the focus of this paper. The following describes the development of questions for the 10-item AHC HRSN screening tool for the core HRSNs.
Housing Instability
Unmet housing needs may include homelessness, poor housing quality, or inability to pay a mortgage or rent. Acknowledging that perception of need may be different for various housing situations, the TEP recommended including examples of homelessness and substandard housing in the tool. After reviewing validated and common housing questions, the TEP recommended inclusion of two questions for this domain (Box 1).
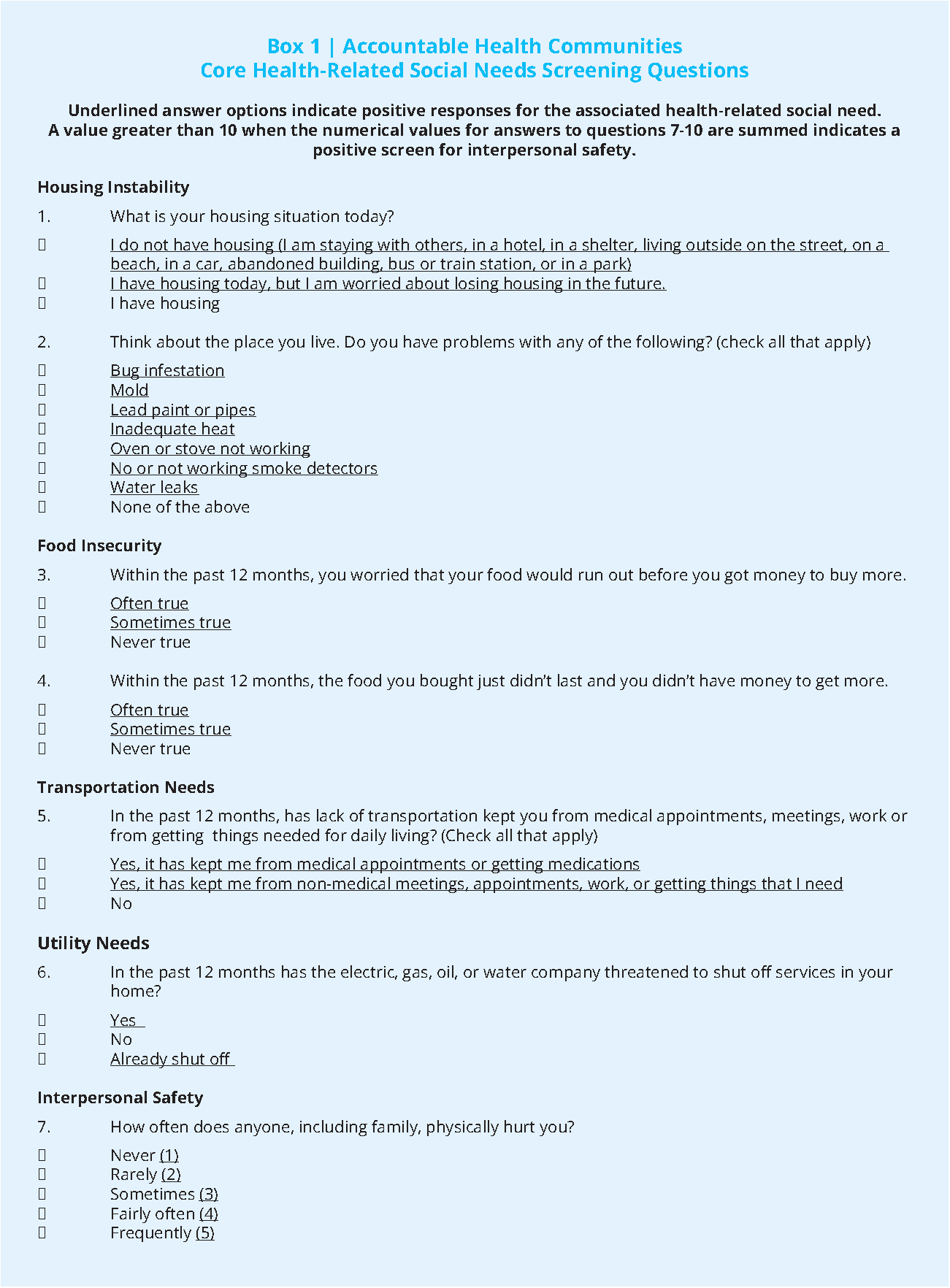

The first housing question is adapted from the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE) assessment tool developed by the National Association of Community Health Centers and partners [15]. The first answer option is intended to identify beneficiaries who are homeless. Accordingly, the TEP recommended adding “abandoned building, bus or train station” to the examples offered to better align with the federal definition of “homeless” [16]. The second answer option is intended to identify beneficiaries who are at risk of losing their housing for any reason, including the inability to pay a mortgage or rent. Selecting either option 1 or option 2 would indicate that the beneficiary has a housing need for the purposes of the AHC Model. The second housing question is adapted from a question developed by Nuruzzaman and colleagues and is intended to identify beneficiaries who are living in substandard housing [17]. Selecting any answer option other than “none of the above” would indicate that the beneficiary has a housing need for the purposes of the AHC Model.
Food Insecurity
The U.S. Department of Agriculture (USDA) defines food security as “access by all people at all times to enough food for an active, healthy life.” The AHC HRSN screening tool will include two questions, recommended by the TEP, to identify food insecurity among community-dwelling Medicare and Medicaid beneficiaries in the AHC Model (Box 1). CMS adapted these questions from the Hunger Vital SignTM, a published two-question food insecurity screening tool that has shown to be sensitive, specific, and valid when asked of low-income families with young children [18]. The American Academy of Pediatrics recommends that pediatricians screen all children for food security using this two-item screening tool [19]. The questions in the two-item screening tool are also part of the full 18-item USDA U.S. Household Food Security Survey [20]. The TEP recommended changes to the introductory text and question stems in order to match the voice of the other AHC screening tool questions. Selecting “often true” or “sometimes true” for either question would indicate that the beneficiary is food insecure or at risk of food insecurity for the purposes of the AHC Model.
Transportation Needs
Unmet transportation needs encompass lack of transportation to get to any destinations needed for daily living. The TEP suggested differentiating between medical and non-medical transportation needs in order to help target the resources suggested during referral and navigation. The AHC screening tool will include one question to identify any unmet transportation needs among community-dwelling Medicare and Medicaid beneficiaries in the AHC Model (Box 1). This question was adapted from the PRAPARE assessment tool. Selecting any answer option other than “no” indicates that a beneficiary has a transportation need for the purposes of the AHC Model.
Utility Needs
When screening for a beneficiary’s difficulty paying utility bills, the TEP recommended listing specific utilities for clarity and adding furnace oil as an example to address regional variation in utilities. After reviewing validated and common questions on utility needs, the TEP recommended one question for inclusion in the AHC HRSN screening tool. This question is adapted from the validated Children’s Sentinel Nutrition Assessment Program (C-SNAP) survey [21]. Selecting any answer option other than “no” would indicate that the beneficiary has a utility need for the purposes of the AHC Model.
Interpersonal Safety
The AHC HRSN screening tool includes four questions related to interpersonal safety, including exposure to intimate partner violence, elder abuse, and child abuse. CMS adapted these questions from the Hurt, Insult, Threaten, and Scream (HITS) instrument, which has been validated in multiple settings around the world for use as a self-report or clinician-administered tool to identify intimate partner violence among women and men [22, 23, 24]. In order to broaden the scope of these questions beyond intimate partner violence, the TEP recommended editing the question stems to say “anyone, including family” instead of “your partner.” The HITS instrument is scored as a whole. Each answer option is numbered sequentially from 1 to 5 points, where “never” is 1 point and “frequently” is 5 points. Thus, scores for this domain range from 4-20. A score of greater than 10 would indicate that the beneficiary is experiencing or at risk of interpersonal violence for the purposes of the AHC Model.
The TEP made special recommendations regarding the framing and placement of the interpersonal safety questions because of the sensitive nature of this topic. For example, the TEP recommended introducing these questions with the following normalizing language: “Because violence and abuse happens to a lot of people and affects their health, we are asking the following questions.” The TEP also recommended that the screening tool ask the questions on interpersonal safety later in the screening to give an opportunity for staff to first build rapport with beneficiaries when they deliver the tool face-to-face.
Discussion
The impacts of unmet HRSNs, such as homelessness, inconsistent access to food, and exposure to interpersonal violence, on health care utilization and individual health are well established [1, 2, 3]. Fortunately, growing evidence indicates that addressing these and other needs can help reverse their deleterious health effects [25, 26, 27]. While some health care systems like Hennepin Health in Minnesota and Kaiser Permanente in California have pioneered efforts to connect members with unmet needs to community services, broader adoption of such programs is contingent on the development of approaches scalable across a variety of contexts [28, 29]. Regardless of the approach, the foundational step to addressing unmet HRSNs is to support clinicians and staff in identifying them, as through the universal application of a clinical screening tool like the one described in this paper.
A growing body of screening tools and surveys has been developed to aid in individual- and community level social needs assessments or population risk adjustments [30, 31, 32]. The AHC HRSN screening tool, however, was specifically developed to identify HRSNs that negatively impact health and health care utilization, and, importantly, can be addressed through community interventions. Furthermore, the tool is unique in that it combines screening across 5 key domains of HRSNs into only 10 questions. Few social need screening tools achieve the same breadth with similar brevity. The AHC HRSN screening tool’s breadth increases the likelihood that significant needs will be identified, as well as presents an opportunity to evaluate the impact of assessing multiple domains at one time. Meanwhile, the tool’s brevity and simplicity enable it to be integrated into crowded clinical workflows while remaining accessible to a diverse group of patients. These qualities support the universal application of the tool to screen all individuals seeking care, thereby reducing the risk of missed unmet needs through provider-triggered
screening [9].
While the attributes discussed above facilitate the clinical application of this HRSN screening tool, several limitations are worth noting. First, the tool’s questions focus solely on the core and supplemental HRSN domains addressed in the AHC Model and do not represent a comprehensive screen of all HRSNs. The 2014 report from the Institute of Medicine (IOM) on capturing social and behavioral measures in electronic health records (EHRs) identified 17 domains that had valid measures that could be incorporated into EHRs [33]. Although most of the domains described in the IOM report are also included as either core or supplemental domains for this AHC HRSN screening tool, others are not included because the domain did not meet the inclusion criteria discussed above. For example, country of origin is a domain identified by the IOM report, but does not qualify as a need that interventions could change, and health literacy is an IOM report domain, but is not commonly addressed by community service providers to which patients could be referred. Second, the questions are broadly worded, limiting the ability to delineate specific types of need within each domain explored. This tradeoff was consciously made in order to identify the largest proportion of clinically significant needs in the fewest questions. Finally, although the tool is based on commonly used or evidence-based questions recommended by an experienced panel of technical experts, several questions have been modified or adapted and have not been tested as a unit and in this format previously, which may impact their validity or reliability. The tool will be delivered in a variety of formats (i.e., both paper-based and electronic, staff-administered and self-screened, and in multiple languages), to a wide range of ages, and in a number of different clinical settings (e.g., primary care clinics, behavioral health centers, and emergency departments). As a result, CMS will monitor the tool’s performance across AHC participants and consider making future updates to its design based on feedback gained through its practical application.
Conclusion
Identifying the burden of unmet HRSNs is the critical first step to connecting individuals to resources in their communities that can address those needs and, as a result, improve their health. The AHC HRSN screening tool was designed to accomplish this function for several key non-medical drivers of health in a way that is broadly applicable across a spectrum of ages, conditions, backgrounds, and settings, while remaining streamlined enough to be incorporated into busy clinical workflows. Applying this tool in the AHC Model will help CMS to evaluate the impact of local partnerships among health care providers and community service organizations—working toward common goals and empowered by shared data and tools—in advancing the aims of addressing the cost and quality of health care across all settings, and safeguarding the health of our nation.

References
- Kushel, M. B., E. Vittinghoff, and J. S. Haas. 2001. Factors associated with the health care utilization of homeless persons. JAMA 285(2):200–6. https://doi.org/10.1001/jama.285.2.200
- Ma, C. T., L. Gee, and M. B. Kushel. 2008. Associations between housing instability and food insecurity with health care access in low-income children. Ambulatory Pediatrics 8(1):50–7. https://doi.org/10.1016/j.ambp.2007.08.004
- Bonomi, A. E., M. L. Anderson, F. P. Rivara, and R. S. Thompson. 2009. Health care utilization and costs associated with physical and nonphysical-only intimate partner violence. Health Services Research 44(3):1052–67. https://doi.org/10.1111/j.1475-6773.2009.00955.x
- Kroenke, K., R. L. Spitzer, and J. B. Williams. 2001. The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine 16(9):606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
- Hunt, S. A., W. T. Abraham, M. H. Chin, A. M. Feldman, G. S. Francis, T. G. Ganiats, M. Jessup, M. A. Konstam, D. M. Mancini, K. Michl, J. A. Oates, P. S. Rahko, M. A. Silver, L. W. Stevenson, and C. W. Yancy. 2009. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 119(14):e391–479. Available at: https://www.ncbi.nlm.nih.gov/pubmed/19324966 (accessed August 25, 2020).
- Ewing, J. A. 1984. Detecting alcoholism. The CAGE questionnaire. JAMA 252(14):1905–7. https://doi.org/10.1001/jama.252.14.1905
- Gottlieb, L., D. Hessler, D. Long, A. Amaya, and N. Adler. 2014. A randomized trial on screening for social determinants of health: the iScreen study. Pediatrics 134(6):e1611–8. https://doi.org/10.1542/peds.2014-1439
- Garg, A., S. Toy, Y. Tripodis, M. Silverstein, and E. Freeman. 2015. Addressing social determinants of health at well child care visits: a cluster RCT. Pediatrics 135(2):e296–304. https://doi.org/10.1542/peds.2014-2888
- Hassan, A., E. A. Blood, A. Pikcilingis, E. G. Krull, L. McNickles, G. Marmon, S. Wylie, E. R. Woods, and E. W. Fleegler. 2013. Youths’ health-related social problems: concerns often overlooked during the medical visit. Journal of Adolescent Health 53(2):265–71. Available at: https://integrationacademy.ahrq.gov/products/literature-collection/literature/youths-health-related-social-problems-concerns-often (accessed August 25, 2020).
- Garg, A., A. M. Butz, P. H. Dworkin, R. A. Lewis, and J. R. Serwint. 2009. Screening for basic social needs at a medical home for low-income children. Clinical Pediatrics (Phila) 48(1):32–6. https://doi.org/10.1177/0009922808320602
- Chung, E. K., B. S. Siegel, A. Garg, K. Conroy, R. S. Gross, D. A. Long, G. Lewis, C. J. Osman, M. J. Messito, R. Wade Jr., H. S. Yin, J. Cox, and A. H. Fierman. 2016. Screening for Social Determinants of Health Among Children and Families Living in Poverty: A Guide for Clinicians. Current Problems in Pediatric and Adolescent Health Care 46(5):135–53. https://doi.org/10.1016/j.cppeds.2016.02.004
- Fleegler, E. W., T. A. Lieu, P. H. Wise, and S. Muret-Wagstaff. 2007. Families’ health-related social problems and missed referral opportunities. Pediatrics 119(6):e1332–41. https://doi.org/10.1542/peds.2006-1505
- Alley, D. E., C. N. Asomugha, P. H. Conway, and D. M. Sanghavi. 2016. Accountable Health Communities–Addressing Social Needs through Medicare and Medicaid. The New England Journal of Medicine 374(1):8–11. https://doi.org/10.1056/NEJMp1512532
- Eggleston, E. M. and J. A. Finkelstein. 2014. Finding the role of health care in population health. JAMA 311(8):797–8. https://doi.org/10.1001/jama.2014.163
- National Association of Community Health Centers, Association of Asian Pacific Community Health Organizations, Association OPC, Institute for Alternative Futures. 2016. The Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE) [Internet]. Available at: www.nachc.org/prapare (accessed August 25, 2020).
- Gubits, D., M. Shinn, M. Wood, S. Bell, S. Dastrup, C. D. Solari, S. R. Brown, D. McInnis, and T. McCall. 2016. Family Options Study: 3-Year Impacts of Housing and Services Interventions for Homeless Families. Washington, D.C. Available at: https://rhyclearinghouse.acf.hhs.gov/library/2016/family-options-study-3-year-impacts-housing-and-services-interventions-homeless (accessed August 25, 2020).
- Nuruzzaman, N., M. Broadwin, K. Kourouma, and D. P. Olson. 2015. Making the social determinants of health a routine part of medical care. Journal of Health Care for the Poor and Underserved 26(2):321–7. https://doi.org/10.1353/hpu.2015.0036
- Hager, E. R., A. M. Quigg, M. M. Black, S. M. Coleman, T. Heeren, R. Rose-Jacobs, J. T. Cook, S. A. Ettinger de Cuba, P. H. Casey, M. Chilton, D. B. Cutts, A. F. Meyers, and D. A. Frank. 2010. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 126(1):e26–32. https://doi.org/10.1542/peds.2009-3146
- Council on Community Pediatrics, Committee on Nutrition. 2015. Promoting Food Security for All Children. Pediatrics 136(5):e1431–8. https://doi.org/10.1542/peds.2015-3301
- Coleman-Jensen, A., C. Gregory, and A. Singh. 2014. Household Food Security in the United States in 2013. USDAERS Economic Research Report Number 173. http://dx.doi.org/10.2139/ssrn.2504067
- Cook, J. T., D. A. Frank, P. H. Casey, R. Rose-Jacobs, M. M. Black, M. Chilton, S. Ettinger de Cuba, D. Appugliese, S. Coleman, T. Heeren, C. Berkowitz, and D. B. Cutts. 2008. A brief indicator of household energy security: associations with food security, child health, and child development in US infants and toddlers. Pediatrics 122(4):e867–75. https://doi.org/10.1542/peds.2008-0286
- Sherin, K. M., J. M. Sinacore, X. Q. Li, R. E. Zitter, and A. Shakil. 1998. HITS: a short domestic violence screening tool for use in a family practice setting. Family Medicine 30(7):508–12. Available at: https://pubmed.ncbi.nlm.nih.gov/9669164/ (accessed August 25, 2020).
- Shakil, A., S. Donald, J. M. Sinacore, and M. Krepcho. 2005. Validation of the HITS domestic violence screening tool with males. Family Medicine 37(3):193–8. Available at: https://pubmed.ncbi.nlm.nih.gov/15739135/ (accessed August 25, 2020).
- Chen, P. H., S. Rovi, M. Vega, A. Jacobs, and M. S. Johnson. 2005. Screening for domestic violence in a predominantly Hispanic clinical setting. Family Practice 22(6):617–23. https://doi.org/10.1093/fampra/cmi075
- Sadowski, L. S., R. A. Kee, T. J. VanderWeele, and D. Buchanan. 2009. Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial. JAMA 301(17):1771–8. https://doi.org/10.1001/jama.2009.561
- Linkins, K. W., J. J. Brya, and D. W. Chandler. 2008. Frequent users of health services initiative: final evaluation report. Available at: https://www.chcf.org/wp-content/uploads/2017/12/PDF-FUHSIEvaluationReport.pdf (accessed August 25, 2020).
- Frank, D. A., N. B. Neault, A. Skalicky, J. T. Cook, J. D. Wilson, S. Levenson, A. F. Meyers, T. Heeren, D. B. Cutts, P. H. Casey, M. M. Black, and C. Berkowitz. 2006. Heat or eat: the Low Income Home Energy Assistance Program and nutritional and health risks among children less than 3 years of age. Pediatrics 118(5):e1293–302. https://doi.org/10.1542/peds.2005-2943
- Sandberg, S. F., C. Erikson, R. Owen, K. D. Vickery, S. T. Shimotsu, M. Linzer, N. A. Garrett, K. A. Johnsrud, D. M. Soderlund, and J. DeCubellis. 2014. Hennepin Health: a safety-net accountable care organization for the expanded Medicaid population. Health Affairs (Millwood) 33(11):1975–84. https://doi.org/10.1377/hlthaff.2014.0648
- Shah, N. R., A. Rogers, and M. Kanter. 2013. Health Care That Targets Unmet Social Needs. NEJM Catalyst. Available at: https://catalyst.nejm.org/doi/full/10.1056/CAT.16.0864 (accessed August 25, 2020).
- Page-Reeves, J., W. Kaufman, M. Bleecker, J. Norris, K. McCalmont, V. Ianakieva, D. Ianakieva, and A. Kaufman. 2016. Addressing Social Determinants of Health in a Clinic Setting: The WellRx Pilot in Albuquerque, New Mexico. Journal of the American Board of Family Medicine 29(3):414–8. https://doi.org/10.3122/jabfm.2016.03.150272
- Takahashi, P. Y., E. Ryu, J. E. Olson, E. M. Winkler, M. A. Hathcock, R. Gupta, J. A. Sloan, J. Pathak, S. J. Bienlinski, and J. R. Cerhan. 2015. Health behaviors and quality of life predictors for risk of hospitalization in an electronic health record-linked biobank. International Journal of General Medicine 8:247–54. https://doi.org/10.2147/ijgm.s85473
- Ridgeway, J. L., T. J. Beebe, C. G. Chute, D. T. Eton, L. A. Hart, M. H. Frost, D. Jensen, V. M. Montori, J. G. Smith, S. A. Smith, A. D. Tan, K. J. Yost, J. Y. Ziegenfuss, and J. A. Sloan. 2013. A brief Patient Reported Outcomes Quality of Life (PROQOL) instrument to improve patient care. PLoS Medicine 10(11):e1001548. https://doi.org/10.1371/journal.pmed.1001548
- Institute of Medicine. 2014. Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 2. Washington, DC: The National Academies Press. https://doi.org/10.17226/18951