Improving Short-Term Medical Engagements with Low-to-Middle-Income Countries

Introduction
The term short-term medical engagements (STMEs) encompasses medical missions, volunteer internships, medical and nursing student rotations, global health education, and medical brigades. STMEs represent a way for faith-based, non-profit, and grassroots organizations, as well as academic institutions and corporations in high-income countries (HICs), to contribute to the health and well-being of people in low-to-middle-income countries (LMICs) through direct provision of health services, donations of equipment and supplies, capacity building, and research findings [13]. STMEs also represent a way for participants to develop cross-cultural awareness and field experience in different country settings.
In 2018, Lasker and colleagues performed a scoping review of the literature on STMEs to determine “core principles for effective and ethical” STMEs [13]. Lasker and colleagues identified the following six core principles:
- appropriate recruitment, preparation, and supervision of volunteers;
- a host partner that defines the program, including the needs to be addressed and the role of the host community in directing and teaching the volunteers;
- sustainability and continuity of programs;
- respect for governance and legal and ethical standards;
- regular evaluation of programs for impact; and
- mutuality of learning and respect for local health professionals. [13]
These principles provide the framework for this paper. We believe that ethics underpins and is embedded within and across all of the core principles. Adherence to these core principles is required for the ethical conduct of STMEs.
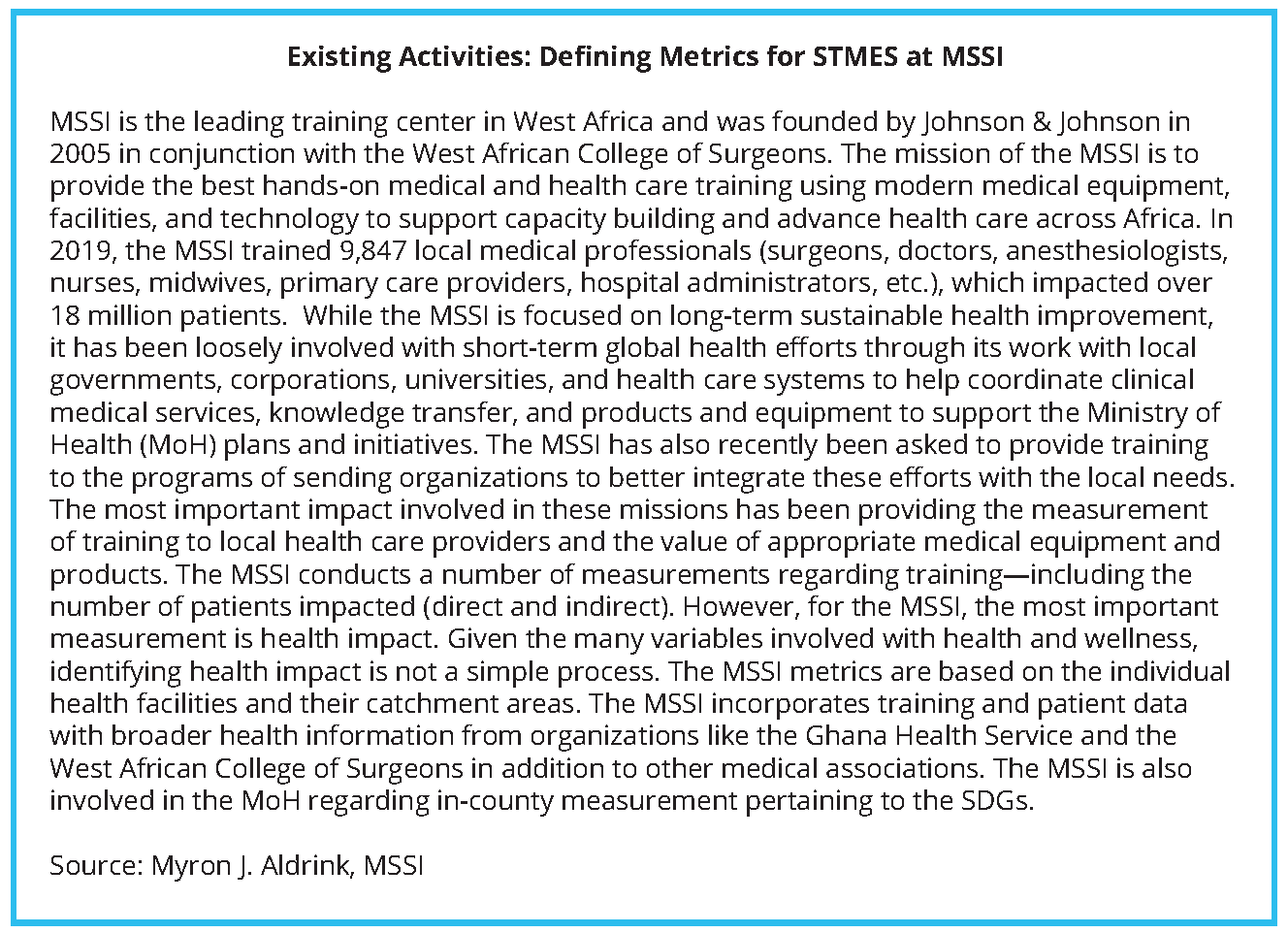
Over the past decades, some STMEs have developed and maintained effective recurring short-term engagements, based on long-term committed partnerships. For example, the organization ReSurge has worked for decades to bring doctors to LMICs to perform reconstructive surgeries; importantly, it began with the request of a local Nepalese doctor to train local doctors in Nepal. The organization has since trained 858 regional medical professionals around the world in surgeries to repair deformed hands; cleft palates; burn scars; and deformed eyelids, ears, and hands. ReSurge reported that local health professionals trained in Africa, Asia, and Latin America performed 91% of the 4,101 procedures sponsored by the organization [21]. STMEs that focus on building capacity while working with and responding to the needs of their host communities, with a long-term commitment, represent the potential for such engagements to positively change the quality and value of STMEs in LMICs. Still, too many STMEs are not guided by the principles and values that lead to ethical partnerships or successful outcomes and, rather than benefit the communities they engage with, have either had no impact at all or have caused harm to either their intended beneficiaries or to their own volunteers [2]. The most egregious examples have resulted in the unnecessary death, injury, or illness of both the so-called “beneficiaries” and volunteers [2]. The sections listed below describe some of the issues found in the literature, through our own observations working in STME coordination, and through insights gleaned from qualitative surveys collected from individuals from the following organizations and academic institutions: Medical and Surgical Skills Institute (MSSI); Merck & Co., Inc.; the Center for Global Health and Social Responsibility at the University of Minnesota; the Department of Sociology and Anthropology at Lehigh University; and the Global Medical Program at Massachusetts General Hospital. Some of the issues within poorly directed STMEs include a lack of coordination with existing medical services and national and local public health officials; language and cultural understanding; medical skill sets (appropriate experience, training, and licensing) to perform procedures; familiarity with national and local laws; knowledge of unique challenges that may affect medication intake (e.g., the availability of food and water); and understanding of individual medical histories and continuity of care.
More broadly, the sections below also illuminate the point that without necessary research and communication with the partner community, some interventions may not necessarily cause extensive harm to individuals, but rather, may be misaligned with the needs of the communities they seek to assist and so are either less effective or unwanted. These engagements represent a lost opportunity in terms of wasting resources that could have been applied to a quality STME or to meet other needs of the partner community and sometimes also waste preciously limited resources of the host community. These failed STMEs rarely become public knowledge. Moreover, the failure may not be recognized or acknowledged by the leaders and participants. Generally, there is little to no oversight, nor is there a requirement for a public record regarding STME activities. Without oversight, STMEs may not be self-correcting.
At the same time, global health promotion and partnerships have been encouraged by the Sustainable Development Goals (SDGs)—specifically SDG-3, which seeks to “ensure healthy lives and promote well-being for all at all ages,” and SDG-17, which seeks to “strengthen the means of implementation and revitalize the global partnership for sustainable development” [25]. As in the example of ReSurge, some effective STMEs have successfully contributed to these goals, especially those that focus on SDG-17’s advocacy for targeted “capacity-building in developing countries to support national plans” [25].
This paper also seeks to define both challenges and opportunities that exist for STMEs and suggests coordinated actions to establish best practices for high-quality STMEs.
Recruitment, Preparation, and Supervision of Volunteers
Challenges
STME teams may include care providers, who are licensed in their own countries, and students or lay volunteers, who are essentially untrained and not qualified to provide clinical care. Rowthorn and colleagues noted that it is not unusual to see high school students with an interest in medical studies take part in surgical procedures, deliver babies, and diagnose patients, while participating in an STME [19]. Recruitment of volunteers with skill sets that are aligned with the needs and goals of the engagement is critical to ensuring the efficacy and safety of the engagement. It is also imperative that such individuals are vetted for maturity and personal shortcomings or other challenges that may cause harm to the volunteer, to the host community, or to the STME team dynamics.
One issue in volunteer preparedness revolves around cultural understanding. A 2019 survey analysis of 87 STME participants composed of health care providers and coordinators recruited from organizations in the southeastern region of the United States, which included nurses, pharmacists, physicians, and others, revealed that 45% of the respondents had little to no knowledge of the host country’s culture before departing on their missions [3]. Cultural differences between host countries and medical volunteers can affect how treatment is welcomed and received and influence the way care is delivered. Such differences may influence the patients’ view of their disease and determine the type of care that they will accept [26]. For example, Wall notes that patients in developing countries may have culturally influenced ideas on the “etiology of disease” [26]. Practitioners need to maintain cognizance
of these differences in the way they develop, communicate, and negotiate their treatment plans with their clients [11,26].
Another barrier to volunteer preparedness is that those (e.g., health care providers, students) participating in STMEs in LMICs often travel to countries where a different language is spoken. For those participants delivering STMEs, lack of familiarity with local languages can impede both medical diagnosis and management, specifically causing issues with obtaining medical histories and educating patients about their medical conditions and medication side effects [18]. In addition, while a good medical interpreter can facilitate the diagnosis process, a poor interpreter without medical knowledge may contribute to inaccurate diagnosis with possible harmful interventions that may not be followed up on, since the medical volunteers may only serve for a limited time [26]. Language and cultural differences may also lead to medical and STME evaluation surveys that have “insufficiently useful or valid” conclusions [12].
Opportunities
The following suggestions may help to remediate some of the barriers to appropriate recruitment, preparation, and supervision of volunteers discussed above:
- Empower and recognize host country supervision of STME volunteers that conforms to the ethical and legal standards defined by host country norms and law.
- Build regionally specific cultural competency materials into pre-departure trainings [10].
- Respect and, where feasible, actualize host country ideas and innovations regarding the STME. This would include during the formation of pre-departure trainings [10].
- Recruit volunteers whose skill sets, personalities, dispositions, and experience align with the needs and goals of the project and its team [20]. If less experienced volunteers are chosen because the STME calls for simpler tasks to be performed, ensure they receive proper oversight from those who have experience specific to the STME.
- Determine (e.g., through interviews, references) whether the volunteer’s primary focus is to contribute to the objectives of the engagement, rather than self-interest (e.g., improving resume, ego, degree requirements).
- Give volunteers a thorough orientation inclusive of developing cultural awareness; broader knowledge of host country politics and economics; and an understanding of regional resource limitations and possible barriers to interventions, including “biological and nonbiological factors that influence the epidemiology of disease” [8].
- Ensure that appropriate compensation for locals working with the STME has been considered, since the time and energy of these locals may be diverted toward supporting the engagement.
- Gauge what the limits should be on the total number of volunteers based on feedback from the host community.
- Ensure volunteer training is inclusive of nonverbal communication and cues that may be unique to the culture of the host community [9].
- Maintain ongoing communication with the host community to determine how they perceive the engagement to ensure appropriate actions are taken to improve the STME.
- Incorporate accountability training that instructs STME participants not to work beyond the limits of their skill sets, certifications, and competence [9] and to distribute the same standard of care considered acceptable in HICs.
- Invest in quality medical interpreters that not only speak the language but also understand and can communicate medical information between STME participants and the host community.
- Ensure the safety of the STME participants through communicating pre-trip vaccination and medical protocols specific to the region, securing safe housing and transportation, and assessing barriers (e.g., communicable diseases, fragile states) that may compromise the security of the volunteers. Determine the inherent health and safety risks of the engagement and communicate those honestly with volunteers.
- Select, prepare, and supervise participants to ensure that the entire team shares the values of the STME.
Partnership with the Host Community
Challenges
The importance of host community engagement in defining STME programs has been noted by the health community at large. According to the World Health Organization (WHO), “Twinning partnerships between health institutions are an innovative approach that can be utilized for improving different aspects of health service delivery” [28]. The WHO Twinning Partnerships for Improvements (TPI) Tools and Resources lay out a six-step process that provide a framework for developing institutional partnerships that include short-term engagements. WHO goes on to say, “The key aim of TPI is to support institutions in the improvement of the quality of their service delivery while aligning with the overall national strategic direction on improving quality of health services.” WHO identifies three objectives to assist in reaching this goal: (1) partnership—fostering strong bidirectional partnerships between health institutions, (2) improvement—bringing changes to improve health care services, and (3) spread—allowing knowledge and learning to flow [29].
Unfortunately, this emphasis and tools on twinning partnerships do not always reach those devising or leading STMEs.
A 2015 survey, orchestrated under the direction of the Catholic Health Association (CHA) of the United States, found that one in four host community representatives had minimal or no involvement in planning the STME [20]. Local providers and community leaders play a critical role in communicating the medical needs of their community, and their lack of involvement in the STME can affect all aspects of the engagement, including priority setting, planning, oversight, patient care, clinical follow-up, evaluation, mutuality, and respect [27]. Those participating in STMEs need to understand the priorities of the host community, and the goals and objectives of the engagements need to be communicated to ensure alignment, success, and safety for all involved. Communication of resource limitations and unique expectations between STME participants and the host community are critical to ensure that such expectations are appropriately managed and aligned.
We have observed that some STMEs may supplant an existing workforce capacity (while directing the local community away from their work to support the STME) and include activities for which the host community has the expertise, but perhaps lacks the financial resources, to execute themselves. If the only roadblock for the community is financial (e.g., for training, medical equipment, and medical supplies), then those on both sides of the STME partnership (host and sending communities) should establish whether their presence is actually essential or whether making a financial contribution to meet that challenge is a more ethical, legal, and economical solution.
Opportunities
The following suggestions may improve the coordination between STME and host community goals:
- Ensure the host community identifies the need and the STME is at the invitation of the host community.
- Commit to and establish a partnership that is equitable and ethical, and continually check back that the guiding principles and values are adhered to.
- Establish alignment between collaborators from host and sending communities with agreed-upon goals and objectives, at the inception of and throughout the duration of the project.
- Engage and involve host community and local health care providers in the planning and implementation of the STME.
- Manage host community and STME participant expectations by communicating resource limitations and setting realistic objectives based on the realities of the STME budgets, timeframes, and human resources.
- Seek advice from representatives of the host community on which health professionals and trainees should be recruited for the STME [15].
- Ensure the needs of the partner require STME physical presence.
- Communicate plans to and seek approval from country and/or local health ministries, either directly or through the host community partner.
Sustainability and Continuity of Programs
Challenges
STMEs have limits on the amount of time engagements are intended to take place, which may have substantial impact on the volunteers’ ability to provide continuity of care or to monitor the outcomes of their interventions. For example, laboratory results (if available) may take longer to obtain than the length of an STME assignment [4]. This lack of continuity can make it challenging to identify potentially harmful practices and more difficult to mitigate complications [4].
In addition, capacity building that may help the host community develop the skills to address their needs is not always seen as a priority for those initiating STMEs. For example, a Lehigh University survey demonstrated that only 22% of those in the sending community perceived host community medical facility capacity building as an important goal [20]. A CHA survey of host community staff revealed that 70% of its respondents indicated that they desired more focus on training local staff [20]. In light of the fact that host community representatives may not want to jeopardize the STME by communicating grievances, this number may be higher.
Opportunities
The following suggestions may improve the sustainability and continuity of programs:
- Establish the STME as part of a long-term commitment to partnership to ensure sustainability.
- Plan STMEs based on what can be accomplished in the period of engagement.
- Build capacity through the STME by working with local communities and providers to design and implement health-focused education and practices.
- Develop sustainability goals in collaboration with host country participants [17].
- Ensure that teaching between STME participants and local providers is bidirectional [17].
- Use locally available resources to ensure the continuity of the interventions after the STME has terminated [15].
- Align donations of pharmaceuticals, medical supplies, and medical equipment with both the needs of the community and their capacity to use and store drugs and supplies and to maintain and operate the equipment [6,27]. It may be important to review the country’s national formulary to ascertain whether patients would have access to the same pharmaceuticals offered during the STME [17].

Legal Standards
Challenges
Laws that require licensing of visiting health professionals or oversight of drug importation are not always inquired about or adhered to by STME participants [19]. However, just as in HICs, most LMIC countries carry strict and punishable laws around practicing medicine without a license [19]. In addition, Rowthorn and colleagues noted that these countries have medical licensure frameworks that require medical practitioners to be either licensed by a professional association or government entity, and while such standards are known to the host country,
“licensed US health care providers often assume, or are told by the US-sponsoring organization, that their US licensure is sufficient. When inquiries are made, many are told that the sponsoring organization or local clinical site is ‘taking care of it’ or that it is too administratively burdensome to get a license, and that engaging in that process will take medical care away from those who need it.” [19]
As noted in guidelines provided by the Association of American Medical Colleges for premedical and medical students, it is critical for the STME volunteers and managers to gain an understanding of local host country laws, regardless of what local health care providers may be communicating about the acceptability of the medical procedures performed during an STME, as violation of these laws may be a punishable offense [1]. Moreover, STME participants (e.g., university-level trainees and high school students) should not undertake activities for which they are not licensed in their own country.
STME participants may not understand the types of visas available to visitors and what they are allowed to do legally under the authority of the visas on which they are volunteering. For example, work on STMEs is not permitted under tourist visas in certain host countries. Other related concerns are that malpractice and liability insurance may be required by the host country to perform health services during an STME, and ignoring these requirements may endanger both the patient and the STME participant. Participants may also arrive with medicine donations (e.g., pharmaceuticals) that have violated the laws of the host country, and these donations include the following:
“medicines that did not comply with locally agreed policies and standard treatment guidelines; donated medicines using trade names that were not registered for use in the recipient country and without an International Nonproprietary Name (INN) or generic name on the label; and medicines donated without the required host country documentation.” [19]
The WHO’s 2003 report, Medical Device Regulations Global Overview and Guiding Principles and its Guidelines For Medicine Donations (revised in 2010) may offer important guidance on such donations. STMEs that include human subjects research may not have properly submitted their research plans for approval by their own institutional review boards (IRBs) or their host countries’ IRBs. Many countries also require that the researchers themselves have permits to perform this research. The landscape for IRB approval, justifiably, has become increasingly time-consuming, rigorous, and expensive in many LMICs.
Opportunities
The following suggestions may encourage respect for legal standards:
- Improve the balance of power between STME participants and their host communities, with more authority and resources directed by local governments and communities.
- Obtain knowledge of host country laws, determine which laws are relevant to the STME, and transmit this information to the STME volunteers, including who can legally practice medicine in the country, medical licenses approval, importation of pharmaceuticals and other medical supplies, work permits, visas, and human subjects research approvals [19].
- Encourage enforcement and development by the host communities and authorities of laws and policies as they relate to the activities of STME participants.
- Uphold the standards of medicine as they are practiced in HICs, inclusive of respect for patient confidentiality and the use of professionals whose training, certification, and skill sets align with the demands.
- Understand the nature and limits of visas and other forms of travel authorization offered by countries hosting STMEs and adhere to all relevant laws and regulations.

Evaluation of Program Impact on Host Community
Challenges
STME program evaluation is critical to assessing its impact and ensuring quality control and patient safety [14] with the ultimate goal of improving the STME. Quality evaluations require resources and time. While many STME partners (host and the sending communities) do not plan for or implement any evaluation [12], those that do may find responses to be skewed or invalid due to cultural differences and language barriers. A survey by the CHA also found some host community leaders feared providing honest feedback to the STME evaluators because they did not want to jeopardize the partnership [20]. These leaders also noted that they rarely saw their feedback incorporated into STME planning efforts, and so it is important that evaluation results are translatable to better practices with the STMEs [20].
Another issue is the often asymmetrical nature of who receives the evaluations. For example, results from one survey suggested that only roughly one in four (27%) from the STME sending community had “ever attempted to evaluate the impact of their activities on host communities,” yet nearly three-quarters of these individuals had evaluated the experience of the volunteers. The lack of incorporation of the host community’s perspective represents an issue that can lead to greater lack of alignment [20]. A CHA survey of the STME sending community found that the “most commonly cited evidence of success was an invitation to return to the same community. Less than 20% of individuals used evidence related to health outcomes” [20]. Another issue is that organizations are measuring impact by counting patient visits or number of people who attend health education classes, rather than health outcomes and knowledge retention. In addition, there is a dearth of published evaluations to assess the effectiveness of STME participant preparatory programs [10]. Such evaluations could enhance understanding how volunteers can best equip themselves for participating in the STME.
Another issue is ensuring that the health outcomes reported align with the needs of the host community. For example, a review of STME literature conducted by Sykes [23] found that the improvements in speech from cleft palette surgeries were of more importance than aesthetic changes in those receiving the STME intervention; however, “speech assessments after cleft lip and palate surgeries were seldom completed and, when they are completed, many reveal[ed] unsatisfactory results” [23]. Furthermore, there is a generalized lack of oversight of STMEs and a parallel lack of reporting of the outcomes, even when they are known. The result is that STME partners (host and sending communities) are not learning, evolving, or improving.
Opportunities
The following suggestions may encourage the regular evaluation of program impact on host communities:
- From the outset, incorporate a plan into STME budgets and management frameworks for evaluation that determines both impact and ways to improve the program.
- Consider cultural differences and language barriers when creating the evaluation and defining outcomes of STME success.
- Consider a cost-effectiveness analysis of STME interventions, which represents a “promising and emerging trend in the development of the evidence base” [23].
- Conduct host community evaluations with the proper assurances that their responses will not negatively affect the partnership.
- Determine what in the STME program represents true impact (e.g., health outcomes).
- Evaluate STME participant preparatory programs to improve participant training and to determine how program impact may be affected by it.
- Respond to evaluations to improve STME quality and effectiveness.
- Share learning and best practices widely to positively influence the larger STME landscape.
- Incorporate host community perspectives through codesigning evaluations or allowing the host community to design the evaluations. Ensure sustainability of the STME interventions are considered when developing impact evaluations.
- Develop impact evaluations that consider the possible negative outcomes of the STME intervention.
Mutuality and Respect
Challenges
The assumed lack of capacity in LMICs can lead to the mistaken belief that the host country will want and appreciate whatever the STME provides. Sullivan, for example, identified two postcolonial racialized tropes in Tanzania that were capitalized on by private volunteer placement organization marketing schemes [22]. The first trope discounts the expertise of local providers, while the second trope envisions “Tanzanian patients as so impoverished that insufficiently trained volunteer help is ‘better than nothing at all’” [22].
In a similar vein, a lack of humility and sensitivity to the needs of the host country’s patients, communities, and local health care professionals is a challenge. In addition, short-term efforts may not build the required rapport with partners and, therefore, while having technical merit, may not be responsive to the LMIC needs. McCall and Iltis pointed to the following five uneven power dynamics and assumptions that may fuel harmful behaviors by the STME volunteers:
(a) offering something always is better than nothing, (b) they or their group are truly going to change a community or be saviors, (c) what they have to offer is better than what local health care professionals or health promoters can provide, (d) volunteering in a different place is a great way to get health care experience, or (e) volunteering is a way to experience a new part of the world. [16]
Finally, STMEs may cause strain on the host community as local health care providers and local resources are used to support the intervention [5]. This diversion of focus and resources may also infringe upon local students’
learning opportunities [5].
Opportunities
The following suggestions may encourage increased respect of volunteers for the country and their partners:
- Establish a relationship that prioritizes equality, respect, and shared decision-making.
- Do not displace in-country providers and administrators.
- Learn from in-country providers and administrators.
- Ensure patients have an understanding of who their care providers are, as well as what their medical qualifications are, and are also informed of, and fully comprehend, their medical diagnosis and treatment options.
- Ensure there is cognizance of the expenditure of resources and time provided by the host community.
Overarching Suggestions for Future STME Development
The concept of “short term” should only refer to the time period of a specific engagement. The STME should not, however, be short on collaboration, quality, planning, supervision, preparation, respect, evaluation, or commitment. Ideally, an STME should be supported by a long-term commitment to a sustainable partnership. While this paper identifies six guiding principles, as well as challenges and opportunities that could be implemented by individuals and organizations participating in STMEs, the authors of this paper believe that systemic progress could come from additional thought and collaboration amongst and between the multitudes of stakeholders. To that end, more input from in-country partners is critical. As STME partnerships are developed or continued, the needs of the host community must be the primary driver, and the activities must align with national health plans and strategies.
As one considers the future of STMEs, there is also an overarching need to evaluate their current activities and ensure that they are ethically executed. Leaders in global health, governments, corporations, nongovernmental organizations, academia, and faith-based organizations should collaborate with in-country partners to identify best practices and develop a set of global guidelines and standards that deliver long-term sustainable, impactful, and efficient STMEs that build capacity and strengthen health systems. Once a set of standards is developed, sectors then need to collaborate to develop tools and resources that will ensure that these standards are followed within and among sectors. All stakeholders should work individually and collectively to create laws, policy, and appropriate shared responsibility to ensure that ethical and legal requirements are met.
As we look towards the future, these actions can contribute to the achievement of the SDGs related to health and partnership.
Join the conversation!
![]() Tweet this! Short-term medical engagements are a manner in which organizations can contribute to the health and well-being of people in low-and-middle-income countries, but must be conducted responsibly and with cultural competency: https://doi.org/10.31478/202103b #NAMPerspectives
Tweet this! Short-term medical engagements are a manner in which organizations can contribute to the health and well-being of people in low-and-middle-income countries, but must be conducted responsibly and with cultural competency: https://doi.org/10.31478/202103b #NAMPerspectives
![]() Tweet this! Authors of a new #NAMPerspectives discussion paper outline challenges and opportunities in improving the effectiveness and cultural competence of short-term medical engagements to ensure the most good and the least harm: https://doi.org/10.31478/202103b #NAMPerspectives
Tweet this! Authors of a new #NAMPerspectives discussion paper outline challenges and opportunities in improving the effectiveness and cultural competence of short-term medical engagements to ensure the most good and the least harm: https://doi.org/10.31478/202103b #NAMPerspectives
![]() Tweet this! “As short-term medical engagements are developed, the needs of the host community must be the primary driver.” Authors of a new #NAMPerspectives identify ways to improve the effectiveness of short-term medical engagements: https://doi.org/10.31478/202103b
Tweet this! “As short-term medical engagements are developed, the needs of the host community must be the primary driver.” Authors of a new #NAMPerspectives identify ways to improve the effectiveness of short-term medical engagements: https://doi.org/10.31478/202103b
Download the graphics below and share them on social media!

References
- AAMC GSA Steering Committee. 2011. Guidelines for premedical and medical students providing patient care during clinical experiences abroad. Available at: https://www.aamc.org/system/files/c/2/181690guidelinesforstudentsprovidingpatientcare.pdf (accessed April 16, 2020).
- Aizenman, N., and M. Gharib. 2019. American with no medical training ran center for malnourished Ugandan kids. 105 died. NPR, August 9. Available at: https://www.npr.org/sections/goatsandsoda/2019/08/09/749005287/american-withno-medical-training-ran-center-for-malnourishedugandan-kids-105-d (accessed April 15, 2020).
- Andrews, S. 2020. Identification of current best practices for short-term medical mission trips and adherence to current common principles and guidelines. Christian Journal of Global Health 7(2):67-82. https://doi.org/10.15566/cjgh.v7i2.341
- Bauer, I. 2017. More harm than good? The questionable ethics of medical volunteering and international student placements. Tropical Diseases, Travel Medicine and Vaccines 3(1):5. https://doi.org/10.1186/s40794-017-0048-y
- Bozinoff , N., K. P. Dorman, D. Kerr, E. Roebbelen, E. Rogers, A. Hunter, T. O’Shea, and C. Kraeker. 2014. Toward reciprocity: Host supervisor perspectives on international medical electives. Medical Education 48(4):397-404. https://doi.org/ 10.1111/medu.12386
- Compton, B., D. M. Barash, J. Farrington, C. Hall, D. Herzog, V. Meka, E. Rafferty, K. Taylor, and A. Varghese. 2018. Access to medical devices in low-income countries: Addressing sustainability challenges in medical device donations. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201807a
- The European Esther Alliance (EEA). 2014. Strategic Framework of the EEA 2015–2020. Available at: https://esther.eu/wp-content/uploads/2018/01/Strategic-Framework.pdf (accessed January 11, 2021).
- Gupta, R., and P. E. Farmer. 2005. International electives: maximizing the opportunity to learn and contribute. MedGenMed: Medscape General Medicine 7(2):78. Available at: https://pubmed.ncbi.nlm.nih.gov/16369456/ (accessed January 11, 2021).
- Johnson, K. L., N. Z. Alsharif, J. Rovers, S. Connor, N. D. White, and M. D. Hogue. 2017. Recommendations for planning and managing international short-term pharmacy service trips. American Journal of Pharmaceutical Education 81(2):23. https://doi.org/10.5688/ajpe81223
- Kalbarczyk, A., E. Nagourney, N. A. Martin, V. Chen, and B. Hansoti. 2019. Are you ready? A systematic review of pre-departure resources for global health electives. BMC Medical Education 19:166. https://doi.org/10.1186/s12909-019-1586-y
- Kleinman, A., and P. Benson. 2006. Anthropology in the Clinic: The Problem of Cultural Competency and How to Fix It. PLoS Medicine 3(10):e294. https://doi.org/10.1371/journal.pmed.0030294
- Lasker, J. 2016. Hoping to help: The promises and pitfalls of global health volunteering. Ithaca, New York: ILR Press.
- Lasker, J. N., M. Aldrink, R. Balasubramaniam, P. Caldron, B. Compton, J. Evert, L. C. Loh, S. Prasad, and S. Siegel. 2018. Guidelines for responsible short-term global health activities: Developing common principles. Globalization and Health 14(1):18. https://doi.org/10.1186/s12992-018-0330-4
- Maki, J., M. Qualls, B. White, S. Kleefi eld, and R. Crone. 2008. Health impact assessment and short-term medical missions: A methods study to evaluate quality of care. BMC Health Services Research 8:121. https://doi.org/10.1186/1472-6963-8-121
- Martiniuk, A. L., M. Manouchehrian, J. A. Negin, and A. B. Zwi. 2012. Brain Gains: a literature review of medical missions to low and middle-income countries. BMC Health Services Research 12:134. https://doi.org/10.1186/1472-6963-12-134
- McCall, D., and A. S. Iltis. 2014. Health care voluntourism: Addressing ethical concerns of undergraduate student participation in global health volunteer work. HEC Forum 26(4):285-297. https://doi.org/10.1007/s10730-014-9243-7
- Roche, S. D., P. Ketheeswaran, and V. J. Wirtz. 2017. International short-term medical missions: a systematic review of recommended practices. International Journal of Public Health 62:31-42. https://doi.org/10.1007/s00038-016-0889-6
- Rovers, J., K. Japs, E. Truong, and Y. Shah. 2016. Motivations, barriers and ethical understandings of healthcare student volunteers on a medical service trip: A mixed methods study. BMC Medical Education 16:94. https://doi.org/10.1186/s12909-016-0618-0
- Rowthorn, V., L. Loh, J. Evert, E. Chung, and J. Lasker. 2019. Not above the law: A legal and ethical analysis of short-term experiences in global health. Annals of Global Health 85(1):79. https://doi.org/10.5334/aogh.2451
- Rozier, M. D., J. N. Lasker, and B. Compton. 2017. Short-term volunteer health trips: Aligning host community preferences and organizer practices. Global Health Action 10(1):1267957. https://doi.org/10.1080/16549716.2017.1267957
- Silberner, J. 2019. Why Surgeons Are Rethinking the Fly-In Medical Mission. NPR, March 27. Available at: https://www.npr.org/sections/goatsandsoda/2019/03/27/656172038/is-it-time-to-rethinkthe-fl y-in-medical-mission (accessed January 18, 2021).
- Sullivan, N. 2018. International clinical volunteering in Tanzania: A postcolonial analysis of a Global Health business. Global Public Health 13(3):310-324. https://doi.org/10.1080/17441692.2017.1346695
- Sykes, K. J. 2014. Short-term medical service trips: A systematic review of the evidence. American Journal of Public Health 104(7):e38-e48. https://doi.org/10.2105/AJPH.2014.301983
- THET. 2017. In our mutual interest. Available at: https://www.thet.org/wp-content/uploads/2017/08/In-Our-Mutual-Interest.pdf (accessed April 20, 2020).
- United Nations (UN). n.d. Sustainable Development Goal 17. Available at: https://sustainabledevelopment.un.org/sdg17 (accessed April 14, 2020).
- Wall, A. 2011. The context of ethical problems in medical volunteer work. HEC Forum 23(2):79-90. https://doi.org/10.1007/s10730-011-9155-8
- Wilson, J. W., S. P. Merry, and W. B. Franz. 2012. Rules of engagement: The principles of underserved global health volunteerism. The American Journal of Medicine 125(6):612-617. https://doi.org/10.1016/j.amjmed.2012.01.008
- World Health Organization (WHO). 2018. Partnership preparation package—A practical guide to implementing twinning partnerships. WHO Twinning Partnerships for Improvement. Available at: https://apps.who.int/iris/bitstream/handle/10665/273158/WHO-HIS-SDS-2018.13-eng.pdf?ua=1 (accessed July 30, 2020).
- World Health Organization (WHO). 2020. Service delivery and safety. Twinning partnerships for improvement. Available at: https://www.who.int/servicedeliverysafety/twinning-partnerships/en/ (accessed November 17, 2020).