Accountable Communities for Health for Children and Families: Approaches for Catalyzing and Accelerating Success

Introduction
Child health is unique. Unlike adults, children are rapidly developing—physically, cognitively, socially, and emotionally. They are highly susceptible to positive and negative interactions with adults, especially parents and caregivers. A child’s epidemiology also differs from adults as they generally have fewer chronic ailments and diseases. Child growth, development, and well-being are distinctly impacted by the communities in which children live, including systems that care for them, such as early care and education, schools, and child welfare systems [1]. Children are especially sensitive to the broader conditions in their neighborhoods—from poverty to inequality to racism to lack
of economic opportunity. These experiences increase risks for chronic diseases and acute events in adulthood, such as mental health conditions, substance use conditions, diabetes, heart disease, and some cancers [2]. All of these unique characteristics necessitate special attention to children’s needs and social and economic context, especially in the early years, in the design of community-based health models and related policy.
Decades of community development literature point to the importance of collaborating with community stakeholders to address the social and economic drivers of health outcomes. Community organizations in a multitude of sectors have a long history of partnering to address these factors—many even with an appreciation of the unique needs of children and families—but the health care sector going beyond its walls to partner with community organizations is relatively new, with some exceptions [3, 4]. The greater alignment among the fields of health care, public health, and community development to sustaining healthy and equitable communities brings new opportunities, resources, and challenges to the table [5].
The authors of this Perspective believe one of the most promising nascent approaches to community-based health emerging from the current wave of health care payment and delivery reform is Accountable Communities for Health (ACHs, as defined here, are distinct from the Center for Medicare & Medicaid Innovation’s Accountable Health Communities (AHC) model, which specifically tests whether systematically identifying and addressing the health-related social needs of Medicare and Medicaid beneficiaries through screening, referral, and community navigation services will impact health care costs and reduce health care utilization) (ACHs). The Funders Forum on Accountable Health (The Funders Forum on Accountable Health is a consortium of public and private health care funders interested in advancing ACH models hosted at the Milken Institute School of Public Health at The George Washington University) defines ACHs as “community-based partnerships formed across sectors such as health care, housing, social services, public health, employment training and economic development to focus on a shared vision and responsibility for the health of the community” [6]. There is growing consensus about the definition and core elements for ACHs and strong agreement that additional effort is needed to build evidence of what works in an ACH, as well as how to sustain and scale them [7]. Currently, only a few ACHs focus on the health and developmental needs of children and families. This could be partially due to the fact that there are special considerations for an ACH focused on children and families that are not faced by an adult-oriented ACH, including fewer opportunities to achieve short-term cost savings and returns on investment (ROIs). However, there is a large body of research indicating that the greatest gains in population health and potential savings in later total health care costs come from investments in early childhood [8, 9, 10]. The relative scarcity of initiatives addressing the unique needs of children in the context of ACHs indicates that additional attention is needed to better understand both the barriers and opportunities facing a proposed ACH for Children and Families (ACHCF).
Defining an ACHCF
An ACH seeking to optimize the health trajectories of children and families in a geographic area over time by improving care and reducing the total cost of care, hereafter referred to as ACHCF, would begin by optimizing the health and well-being of parents and caregivers. Consistent with the approach described by the National Academies of Sciences, Engineering, and Medicine [11], optimizing health outcomes also necessitates a focus on important life periods such as preconception, prenatal, and postpartum periods, and on into childhood and adolescence. The ACH model requires a community coming together around a shared vision and outcomes for which they are all held accountable. In this model, all members of the community have joint responsibility for achieving shared goals and cross-sector metrics, with an integrator organization or organizations serving as a neutral convener that coordinates the effort and acts as the glue that binds the initiative [12]. Based on the work of a year-long Collaborative (described below), this paper describes accelerators, barriers, and potential approaches that can enable the successful adoption of such an ACHCF model.
Additional Foundational Definitions
Two-generation, or “2Gen,” approaches are policies and efforts that simultaneously address the needs of children and their adult caregivers to improve outcomes for the family (including non-biological caregivers). As articulated by Ascend at The Aspen Institute, the five core principles that underlie the 2Gen approach are (1) measure and account for outcomes for both children and their parents, (2) engage and listen to the voices of families, (3) foster innovation and evidence together, (4) align and link systems and funding streams, and (5) ensure equity [2].
A “portfolio of interventions” refers to aligned and mutually reinforcing interventions in a community. These interdependent interventions can include policies, programs, practices, and investment priorities [9]. Taken together, the portfolio should include interventions with different time horizons and levels of risk, encouraging investments across a set of interventions that can collectively affect change inter-generationally, rather than focusing on a single intervention. This creates room for innovative approaches that may yield results in the short, medium, and long term.
For the purposes of this paper, we are linking these two concepts. A distinguishing feature of an ACHCF is that its portfolio of interventions includes a 2Gen lens. Accordingly, an ACHCF includes a suite of interventions across a community intentionally designed and coordinated to reach the whole family over time and recognize that the child is part of a family system. It can include interventions designed to address immediate needs, as well as strategies to optimize health over the long term.
Background
Although most children are healthy, the foundations of health throughout the life course take root in the earliest years [13]. For example, the frequently cited adverse childhood experiences study found that events in childhood were predictive of adult chronic health conditions more than 40 years later [14]. The salience of early experiences and exposures on health and well-being have since been replicated and reaffirmed across a number of studies, and this literature continues to grow [15]. Numerous studies also demonstrate health and behavior effects as early as in utero and infancy, and how intervention in early childhood can reverse these trends and better produce health equity as children grow and develop [16, 17].
Children are dependent on and nurtured by adults, primarily the adults in their families. Research has indicated a strong connection between parents’ economic, psychological, and social well-being and children’s healthy development [18]. For example, a parent’s educational status is a strong predictor of a child’s success, having both direct and indirect impact [19]. Caregiver interactions and parent-child relationships are also critical for nurturing the healthy cognitive, affective, and behavioral development of the child. In addition to reducing or mitigating stressors that can detract from these relationships, health care can also intervene to build on these interactions directly and improve later health outcomes [20, 21]. Approaches that separately address the needs of children and their caregivers miss opportunities for strengthening their interactions, thereby reducing the likelihood of success for the entire family [22]. 2Gen or multi-generational strategies for supporting children and their families offer a critical method of intervention for improving long-term health and well-being.
Community and place also matter for children. Poor, vulnerable, and minority children disproportionately (and by some measures increasingly) live in neighborhoods with far less social, physical, economic, environmental, educational, and employment capital than their peers [23]. Studies increasingly find that this community context is predictive of a child’s developmental outcomes, even independent of the immediate family’s socioeconomic status [24]. While there have been periodic investments made and attention given to place-based strategies to respond to community disinvestment, most have focused on material and economic and workforce issues, and many have not been conducted at a scale that could realistically produce population-level impacts. Because “poor neighborhoods are rich in young children” [25], there is an opportunity to advance efforts to develop place-based approaches that specifically look at community building from a young child perspective. ACHs that are supported by strong anti-poverty policies and designed with a 2Gen focus offer the potential to address social determinants of health and improve outcomes for the full range of community members, including children and families.
Finally, it is critical to acknowledge the role of broader social, economic, and racial issues on child health, including, for example, the impact of racism and economic inequality on black infant mortality [26]. In fact, the National Academies’ 2019 report titled A Roadmap to Reducing Child Poverty stated that “the weight of the causal evidence does indeed indicate that poverty itself causes negative child outcomes, especially when poverty occurs in early childhood or persists throughout a large portion of childhood” [11]. Additionally, many programs that alleviate poverty have been shown to improve child well-being (e.g., earned income tax credits, the Supplemental Nutrition Assistance Program, and the Women, Infants and Children Program) [27]. It is therefore clear that social and economic context and the policies that shape it matter for children.
To explore the promise of an ACHCF model in response to this growing evidence on the context for healthy development in children, on November 1, 2016, Nemours Children’s Health System (Nemours) and the Health, Medicine and Society Program of The Aspen Institute co-convened a meeting to articulate core elements of an ACHCF with experts from academia, children’s health care, government funding agencies, foundations, public health, and children’s health advocacy. Representatives from Nemours synthesized key findings from that meeting, along with additional information from expert interviews, into a Discussion Paper published by NAM Perspectives in 2017 [12]. Subsequently, Nemours, the Scattergood Foundation, and Mental Health America (MHA) submitted a paper to the Center for Medicare & Medicaid Innovation that applied a behavioral health focus to an ACHCF [28].
Ongoing efforts to share best practices and lessons from emerging ACH initiatives can further support ACHs in serving the unique needs of children and families. To this end, Nemours and MHA initiated the Collaborative on Accountable Communities for Health for Children and Families as an activity of the Forum for Children’s Well-Being at the National Academies. The goal of the Collaborative is to examine policies, practices, and recommendations that improve child health trajectories, including practices within the health care setting that effectively refer and connect children and families to developmental and social supports, as well as improve community environments. During its first year, the Collaborative engaged with leading communities and its expert members. In this Perspective, several individual members of the Collaborative propose approaches to governmental and private funders and
policymakers to advance this work.
Methods
Nemours and MHA initially recruited 40 representatives, beginning in Summer 2017, to join the Collaborative, including individuals who participated in the earlier Nemours–The Aspen Institute convening. The recruitment was balanced to ensure diverse perspectives across policymakers/government agency representatives, foundations, child health researchers, child health providers, child health advocates, and leaders in nascent ACHCFs.
In late 2017 and early 2018, Nemours and MHA conducted an initial series of semi-structured interviews with selected members and communities to discuss the core elements of an ACHCF, followed by a survey of all Collaborative members. Using the process described below, Collaborative members refined these proposed core elements, both as a whole and then through deeper analysis of five individual elements that were each featured on themed calls with community presenters, sharing their challenges and successes:
- An overview of the revised core elements,
- Closed loop community care coordination systems,
- Portfolio of interventions and two-generation strategies,
- Financial sustainability, and
- Feedback on synthesis and recommendations.
Based on this input, Nemours and MHA refined the core elements, ensuring that the child/family lens was applied. Specifically, 2Gen approaches were identified as a distinct core element of an ACHCF, and the core element related to the key portfolio of interventions was modified to reflect alignment with family-centered care. Attention was paid to ensuring that both child and family stakeholders and payment models were included and that there was an emphasis on the inclusion of 2Gen approaches.
The Collaborative on Accountable Communities for Health for Children and Families officially launched in April 2018. In its first year, Collaborative members were convened over five virtual meetings. Each call began with an expert presentation offering a conceptual foundation of why the element(s) are proposed as core to an ACHCF, with an opportunity for questions and comments. Leaders from two to three community or state initiatives building ACHCF-type models offered key learnings related to the element(s) in question, highlighting their experiences and the accelerators and barriers to their success, followed by questions from Collaborative members. Community presenters included participants in ACH initiatives; local leaders identified by the Funders Forum on Accountable Health; and others recommended by Collaborative leadership or members.
Nemours and MHA produced summaries of each call with key findings and emerging themes and then synthesized findings into proposed approaches for funders and policymakers interested in advancing ACHCFs. These findings were presented for initial feedback from Collaborative members. Using an iterative process, additional rounds of feedback were solicited from Collaborative members and community presenters to create a final document. This paper synthesizes the lessons shared by Collaborative members and other stakeholders, with a focus on accelerators, barriers, proposed approaches for funders and policymakers, and key questions for communities to consider.
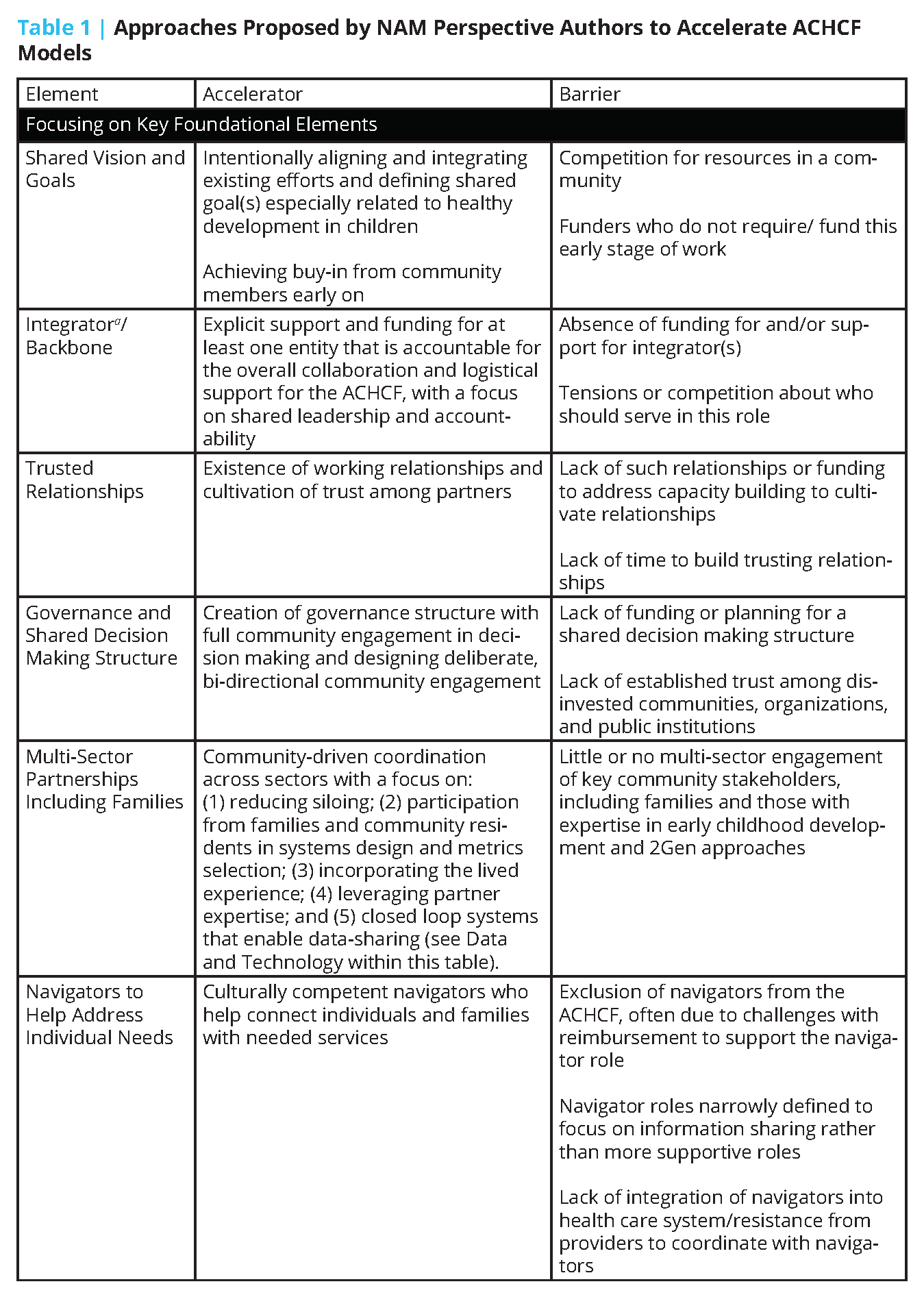
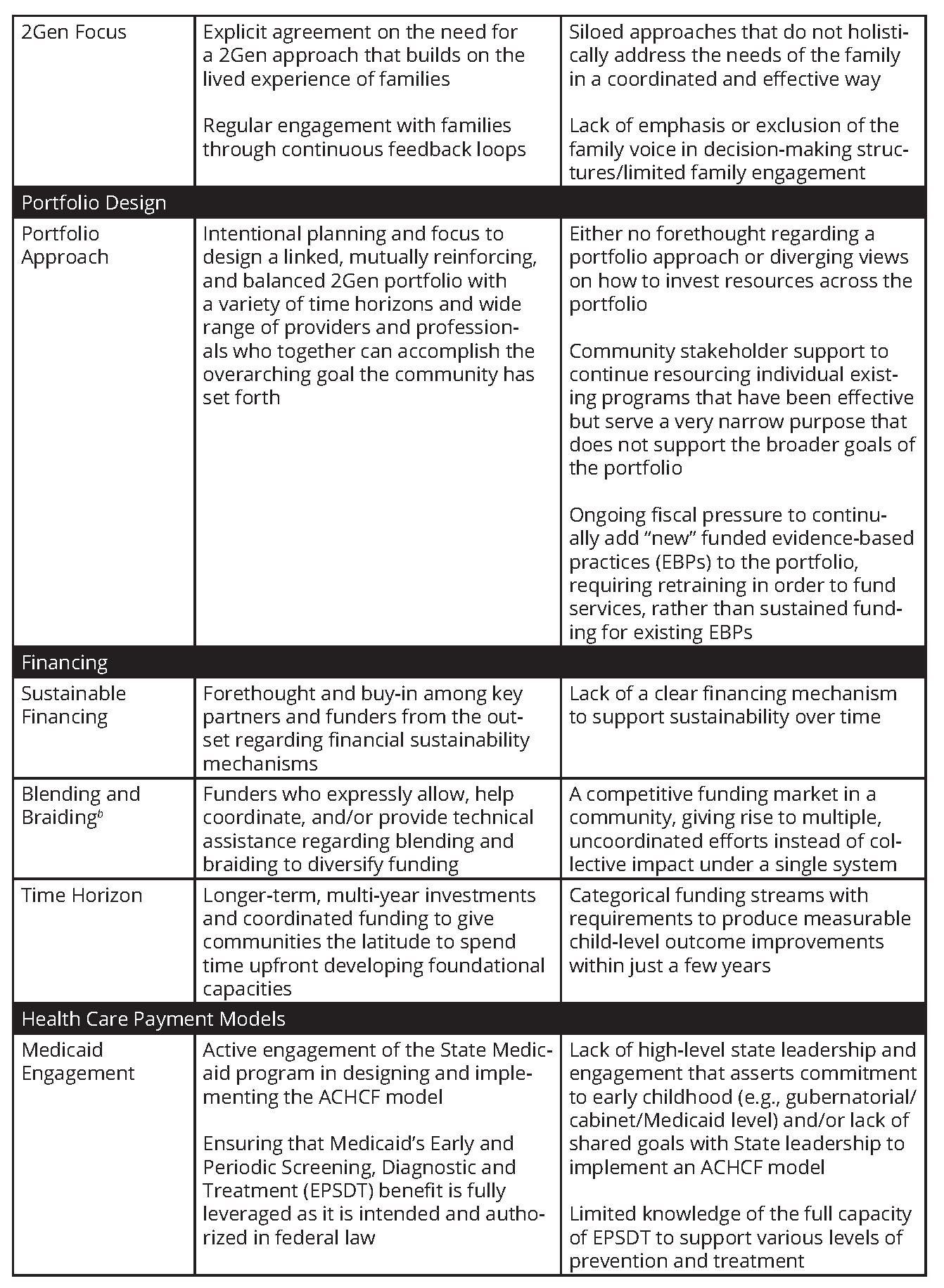
Findings: Key Accelerators and Barriers to ACHCF Models
The following elements emerged as central to catalyzing and sustaining an ACHCF. They are presented alongside key accelerators and barriers that relate to each element. Many of these elements are also relevant to a broader ACH, and communities should be intentional about applying a child/family lens when designing and implementing these elements for an ACHCF. Elements are organized by thematic areas, including (1) focusing on key foundational elements; (2) portfolio design; (3) financing; (4) health care payment models; (5) data and technology; and (6) metrics. The approaches proposed by the authors of this Perspective in the section that follows further define and elaborate on these six areas.
Proposed Approaches
To amplify the accelerators and reduce the barriers identified above, Nemours and MHA have developed the following proposed approaches, gleaned from the Collaborative’s activities, and informed and refined based on input from Collaborative members. The following approaches are intended for community practitioners, public and private funders, federal policy makers, and states.

Focusing on Key Foundational Elements
Successful long-term partnerships are the basis of an ACHCF. They must be cultivated over time and require a strong foundation grounded in trust, shared goals, and processes and governance structures that promote sustainability. These partnerships extend beyond individual institutions and into the community and embrace a whole-child, life-course approach. Funders can support communities in doing the following:
- Create a culture of distributed leadership and establish collective impact. Equip ACHCFs with empirically informed and theory-driven approaches to engaging communities in building their collective structures, setting their vision, distributing leadership at multiple levels, and promoting their success.
- Support communities in developing measures of shared goals that are relevant to children and families upfront. This includes identifying process and outcomes measures at the individual and population level. For example, New York established a Children’s Health Value-Based Payment Subcommittee and Clinical Advisory Group to bring a uniquely child-focused perspective to payment reform. This group established a values statement, guiding principles, and North Star Framework from which further strategies and initiatives cascaded [29].
- Align sectors that care for children and families. Fund locally responsive and inclusive collaboration across sectors to develop a common vision and shared goals. This may represent a change for community stakeholders and/or funders, as many have historically focused on health, education, or juvenile justice, rather than the intersection across systems [5].
- Equitably engage whole communities and establish accountable processes, with an intentional focus on engaging families directly. Fund time to equitably engage community leaders as well as community members to build a culture of inclusivity and accountable governance that is reflective of the lived experience and includes explicit shared decision-making structures with meaningful family engagement. For example, in Boston, the Vital Village community of practice supports the co-creation and design of innovations between residents and community- based agencies with a focus on shared accountability [30].
- Provide ongoing support for navigators who connect individuals with community-based services, as well as a backbone/integrator organization(s) that supports systems-level change across the community and promotes continuous learning and improvement functions. Provide financial and infrastructure/organizational support for backbone/integrator organization(s). Support sufficient time and defined roles for navigators to do more than make referrals [31].
- Support rapid cycle learning through technical assistance (TA), convening, and evaluation. A menu of TA options, grounded in understanding of the ACHCF model, and available when local timing is right can accelerate progress. Supporting evaluation can externally validate local progress and help inform communities about future efforts.
In developing shared goals, communities should consider the following:
- What stakeholders need to be engaged to ensure an equitable approach that promotes the health and well-being of children and families? What key community partners should be engaged (e.g., parents, adolescents, schools, child care, etc.) in design and implementation?
- What are the ways to gain momentum through a series of short-term wins to build cohesion in the group and offer steady progress toward the larger goals?
- What type of governance structure can be put in place to establish accountability among partners and ensure a direct voice for community residents, including children/adolescents and families?
- What shared results and results-based accountability are important and can be measured?
Building a Portfolio of Interventions with a 2Gen Approach
As noted above, a balanced portfolio approach considers a strategy of investments that bring returns over different time periods, and includes health investments that ensure social, economic, and environmental conditions vital to improving overall population health [32]. While specific interventions may show an ROI and have a core of supporters, better health and health equity for children and families will not be the result of layering on a single new intervention. In addition, because the financial benefits associated with many developmentally focused investments in childhood may take decades to fully accrue, stakeholders will need to apply a new paradigm to ROI, as opposed to the one typically used when evaluating business or public investments. To encourage systemic change over time, a broader 2Gen approach that looks across a portfolio of linked interventions should be applied and intentionally integrated into the existing work so it is sustained.
Private and public funders as well as government entities at all levels—local, state, and federal— should leverage their convening power and invest in funding basic organizing functions and capacity building. This includes funding communities to set a common agenda that embraces a portfolio approach, as opposed to singular interventions.
In particular, funders can do the following:
- Build toward a cross-sector 2Gen strategy rather than funding stand-alone interventions that advance narrowly targeted goals. This will ensure that the portfolio is integrated into a larger overarching framework and existing infrastructure. Funders of all types can help grantees in a collective impact arrangement implement cross-sector strategies designed around children and families that use all available policy levers, rather than implementing a single intervention or collaboration that advances a specific goal. For example, Colorado’s Department of Human Services employs a 2Gen approach across its services and encourages its programs to serve children and their caregivers together in order to harness the family’s full potential [22].
- Ensure that the 2Gen strategy and portfolio strengthen the parent-child relationship and that approaches align with various developmental stages (child/adolescent), in addition to systems that influence these developmental stages. According to the Harvard Center for the Developing Child, for children, responsive relationships with adults promote healthy brain development and provide buffering protection needed to prevent very challenging experiences from producing a toxic stress response [33]. A comprehensive strategy includes a diverse portfolio of interventions that entail families, child care, schools, and other community partners
- Apply and build evidence for portfolio management. Equip grantees with empirically informed and theory-driven approaches to portfolio planning, implementation, and management, in addition to helping to evaluate innovations in portfolio management to inform future efforts.
- Test different sustainable financing mechanisms that include a 2Gen approach. This should include innovation related to the source of funding, as well as the mechanism.
- Ensure the portfolio of interventions is balanced in terms of the time horizon for achieving goals and the mix of interventions included. Prior work has indicated that the mix of interventions should be tailored to meet the community’s needs and balanced in several dimensions, including time frame, level of risk, and target population [31]. As they work with communities to build a balanced portfolio, funders should help communities transform their current activities to align with the investment strategy—including strategic reprogramming that reapplies talent and resources in other ways. Funded activities and evaluations should acknowledge that returns may be long term.
- Provide longer-term, multi-year investments to account for the amount of time for coordinating and engaging the community in developing the balanced portfolio, as long-term transformation is challenged by short-term funding horizons. Some interventions may have short-term returns (1–3 years). Others will need a time horizon that could extend beyond 10 years. Funders should work with communities to examine the evidence base and time horizon for interventions and invest, much like in business, in a balanced portfolio with returns over time. For example, New York’s value-based payment guiding principles explicitly state, “Maximizing the healthy growth and development of children today will reduce future health care needs and bring long-term value to Medicaid and other public systems, including but not limited to education, child welfare, and juvenile justice. For
these reasons a longer horizon for assessing cost savings must be considered” [29]. Additionally, the Washington State Institute for Public Policy offers ROI estimates for the Washington State legislature and finds impressive returns for many programs (ROIs of $2:1 or even $3:1 over time), but with varying time-horizons [34]. As a final example, Parent-Child Interaction Therapy for families in the child welfare system shows positive returns within 5 years, whereas investments in high-quality early childhood education can take as many as 20 years to offer positive returns, but across a much larger population.
In implementing 2Gen portfolios, communities should consider the following:
- What programs should be included in the portfolio, and over what time frame should results be expected? What are the most strategic investments to achieve the overarching goals and what programs should be discontinued or revamped because they serve a more siloed purpose? As the portfolio mindset is embraced over time, how can new programs be catalyzed, and how can a balanced portfolio help to minimize the risk of new innovations? What pathways can be initiated for individuals and institutions to reengage if their program is discontinued?
- How do funded programs, policies, and practices consider the family as the unit of action?
- How are families incentivized and empowered to participate actively in portfolio interventions?
Financing Mechanisms to Support Longer-Term Investments
In many cases, individual funding streams are not sufficient to support the array of activities needed to effect change in multiple sectors over time. As a result, leveraging funds from multiple sources in support of an overarching strategy or linked portfolio of interventions can be an effective strategy, although grantees must ensure they are following all federal or state requirements or seeking and receiving explicit permission for an exception to such requirements. For example, blending (i.e., funds are combined into a single pool from which they can be allocated) and braiding (i.e., funds from various sources are pooled together but tracking and accountability is maintained at the administrative level), or a combination of the two, are financing strategies that can help to provide adequate support for strategies in each portfolio category [35]. Blending and braiding and other coordinated funding mechanisms can also help to address “wrong pocket issues” where one agency bears the cost for a program that ultimately results in a reduced demand for services by another agency or system [36].
To assist communities, private and governmental funders, including states, can do the following:
- Support financing mechanisms that promote shared accountability and goals. The authors of this Perspective see opportunities for federal and state funders to collaborate across agencies to facilitate coordinated funding that rewards collective impact and collaboration, with a focus on optimizing health and healthy development. This should include joint investments in capacity and infrastructure needed across sectors to make collective impact effective, as well as setting aside funding for the development of community-based financial sustainability structures such as wellness trusts. An example of an innovative financing mechanism is the Imperial County Local Wellness Fund, which weaves existing resources together to seamlessly and more effectively support community-designated solutions, including solutions to treat and prevent asthma in children.
- Support and provide TA to awardees on blending and braiding funds with the goal of advancing 2Gen efforts across an aligned portfolio of interventions. This includes providing TA on the legal aspects of data-linking
or cross-sector contracting or highlighting examples of and disseminating learnings from communities that have effectively blended and braided funds. For example, the Health Resources and Services Administration’s Early Childhood Comprehensive Systems and Supports initiative provides opportunities for TA and shared learning on braiding and blending for sites interested in addressing both maternal and child early developmental needs. - Apply and build evidence for braiding and blending. Equip grantees with empirically informed approaches to effectively using blended and braided funding, as well as help evaluate innovations in blending and braiding to inform future efforts. The Brookings Institution and the Urban Institute have begun a project that highlights the research of experts in health care financing focused on creative approaches [36]. Funders can help to highlight what we have learned from existing efforts like these and continue to build the evidence base through further research.
- Work with communities and researchers to test methods for conceptualizing and calculating ROI across programs and sectors, especially when blended or braided funding strategies are employed. Investments in programs in one sector (e.g., early care and education or schools) may lead to cost savings and improvements in another sector (e.g., juvenile justice). Developing methods to calculate cross-sector savings can help to build the case for more coordinated cross-sector funding streams that reap benefits across a number of domains.
In implementing financing strategies such as braiding and blending, communities should consider the following:
- What relationships need to be cultivated from the outset to ensure a focus on financial sustainability (e.g., public and private payers), and how can integrator(s) catalyze and sustain the work? How can communities bring funders to the table early to discuss how funds can be more effectively leveraged to achieve community goals?
- How can community partners be engaged in discussions about the options and advantages of braiding and blending funding?
- How can resources and rewards be shared in a way that reduces rather than accelerates competition among local entities? What financing mechanisms (e.g., wellness trusts or social impact financing) could be tested to align with the metrics included in value-based payment models tested within the community?
Testing Value-Based Payment Models to Improve Health and Well-Being for Children and Families
To optimize child health and well-being, financial incentives across health care and other sectors should be aligned with a long-term, 2Gen perspective that rewards whole-family healthy development [37]. This is an emergent area. Further testing is needed of pediatric and/or dyadic (parent/child) payment models to address health-related social needs (e.g., food, housing, child care, etc.) for children and families, and aligned financial sustainability mechanisms [38]. The Center for Medicare and Medicaid Innovation’s Integrated Care for Kids (https://www.cms.gov/newsroom/fact-sheets/integrated-care-kids-in-ck-model) model will be informative as the model is implemented over time.
In particular, and with the evidence that currently exists, funders and/or policymakers can do the following:
- Catalyze testing of multi-payer alternative payment models to address the needs of the pediatric population. Encourage a shift in mindset to embrace payment models that reward value and outcomes. Funders and/or policymakers can catalyze testing of pediatric and/or dyadic payment models that tie value-based payments to measures related to improvements in healthy development and parental mental health, offer incentives to sectors other than health care for their contributions to health, and reinforce shared accountability across sectors.
- Ensure that Medicaid and its Early and Periodic Screening, Diagnostic and Treatment (EPSDT) benefit are used as they are intended and authorized in federal law. Implementation of this approach could include identifying innovative and best practices in how to fully leverage the EPSDT benefit that can be further disseminated [39]. Consider using the Bright Futures guidelines [40] and high-performing medical home design to implement state-of-the-fi eld EPSDT well-child preventive visits. Implementation could also include setting an agenda and priorities for using Medicaid to promote health and positive healthy trajectories. For example, the New York State First 1,000 Days in Medicaid initiative developed a top ten list of priority action areas for using EPSDT to improve care and results [41, 42].
- Recognize that value-based care is not “cost containment” care and must be recognized in that light. The focus should be on improving outcomes. Particularly for preventive and developmental approaches, current financing does not address what the science shows produces improved child health and adult health trajectories. Funders should consider investing in economic modeling and benefit-cost estimation in order to assign value to prevention in terms of long-term costs.
- Ensure public and private payers and managed care plans are engaged early in the process of a community coming together. Work with communities and states to engage state Medicaid program staff, managed care, and private payers from the start of any collaboration and continue to engage them over time, including testing models that include allied health professionals that can help to strengthen the parent-child bond.
Communities should consider the following:
- What untapped potential exists within Medicaid EPSDT benefits, and is EPSDT being fully leveraged and administered equitably by Medicaid, managed care, and mental health plans? How can primary care providers, including federally qualified health centers, children’s hospitals, and other pediatric medical homes be incentivized to optimize quality through innovative payment models?
- How can communities partner with states to develop innovative models and data integration pilots—leading to systemic change—and leverage existing Medicaid authority and Section 1115 Medicaid waiver authority?
- How can communities ensure a focus on the sustainability of a multi-sector system rather than an insular focus on the health care system alone? What funders and other financing stakeholders need to be invited to the table early to inform the design of the ACHCF portfolio and help articulate how to deliver value across sectors over time?
Leveraging Integrated Data and Technology
Data and technology fuel the health care of today and tomorrow. There is promising work at the state level regarding data and technology advancements that can support the creation and maintenance of ACHCFs. For example, the Integrated Data Systems Project, the Early Childhood Data Collaborative, the national Data Quality Campaign, and the Workforce Development Quality Campaign are working to integrate data systems to align with 2Gen efforts [42]. At the federal level, integrating that data and leveraging technology to more seamlessly connect children and families to the services they need continues to be a challenge [38].
To address this challenge, funders and/or policymakers can do the following:
- Support the development of and provide TA regarding a data strategy that includes appropriate data sharing and integration across sectors, with an intentional effort to include child-serving sectors. The authors of this Perspective believe funders should provide TA and financial support for states and communities to achieve appropriate data sharing and integration across sectors, including investing in data systems integration and innovative data system development to better track and report family outcomes. Funding Opportunity Announcements and other opportunities could require or incentivize appropriate data sharing among family-serving grantees to expedite linkages. The Data Across Sectors for Health (DASH) Project includes helpful resources for communities [43].
- Support the adoption of accessible community care coordination systems that “close the loop” and ensure that the information/data is recorded in a way that can be shared across stakeholders, in accordance with privacy laws. The authors of this Perspective encourage governmental and private funders, as well as payers, to continue to invest in and catalyze innovation related to community care coordination systems that are inclusive of children and families. This could include funding a process for cross-sector planning and adoption of a system (ensuring that health and social providers are engaged in the selection of the system and trained in how to use it), funding for a backbone organization to sustain and enhance an existing system, or funding that could be pooled with other streams to maintain the system, including perhaps leveraging large private investments made in them by funders and health systems (e.g., Kaiser Permanente’s investment in the Unite Us system [https://www.modernhealthcare.com/care-delivery/kaiser-launchsocial-care-network]). Closed-loop systems help provide connections to needed services for community members [44]. For example, the Family Connects System (http://www.familyconnects. org) is a home visiting model in which a registered nurse assists families with new babies in connecting to community resources based on identified needs. Similarly, the Help Me Grow model (https://helpmegrownational.org) ensures that communities identify vulnerable children and links families to community-based programs and services.
Communities should consider the following:
- How are the social needs of children and their families identified, and what data and technology systems can help support referrals to address those needs? If it is not feasible to purchase a technology platform, how can partners across sectors maximize coordination even in the absence of such a system?
- How can community buy-in from health and social service providers, and the clients who use those services, be achieved in order to coalesce in support of a community care coordination system that leverages technology to help meet unmet needs?
- What investments, infrastructure, and other changes are needed to facilitate data sharing across sectors?
- What are pathways for working with managed care organizations to invest in closed loop technology systems and incentivize completion of referral pathways?
Selecting Metrics and Evaluating Progress
ACHCFs engage communities to set and meet shared goals for whole-family healthy development and wellbeing. Measurement and evaluation should reflect this. Measurement systems should cut across funding streams to consider the family system. This means moving beyond program-specific measures that are solely child-focused or including only minor attention to parent and caregiver measures. An ACHCF intentionally disrupts current siloed program implementation and measures of success. Therefore, ACHCF evaluation design also needs to reflect principles of learning and quality improvement to inform progress toward the overall goals set by the community and reinforce new ways of interacting and making decisions for collective impact.
Funders can:
- Reinforce the need for the community to set shared goals and a data strategy upfront and use them as guideposts when making future decisions regarding strategy and interventions. Funders can help grantees to collaborate with the community to set goals and milestones, as well as the data strategy to enable this process, so that stakeholders feel ownership over and are interested in working together on the initiative. For example, the California Accountable Communities for Health Initiative developed readiness assessment guidance and tools as well as initiative-wide milestones to encourage this type of effective collective impact.
- Educate grantees about what types of data can and cannot be shared, including best practices for data sharing. Share examples of bright spots and exemplars of communities that have developed data-sharing agreements that are compliant with the Health Insurance Portability and Accountability Act, the Family Educational Rights and Privacy Act, and other privacy laws [43, 45].
- Collaborate to reinforce or allow flexibility for a set of common metrics for grantees that span sectors for collective impact in an ACHCF, track 2Gen impacts, and are reflective of the goals set by the community. Be flexible in the type of evaluation that is required for 2Gen initiatives, allowing for short- and longer-term metrics that capture the functioning of family systems. Work to align metrics with existing efforts, such as the emerging Pediatric Vital Signs (https://sites.nationalacademies.org/DBASSE/ccab/DBASSE_184699) initiative.
- Ensure that investments in the community allow for continuous evaluation of salient outcomes to promote the sustainability of an initiative. Evaluation should include both child and family-focused metrics (with linking between child and parent data) covering health and wellbeing across domains as appropriate.
- Build capacity use data for action as an effective element of a comprehensive evaluation strategy. Pay for and provide TA on effectively sharing data stories with the engaged sectors as well as political leadership for the area in order to promote ongoing sustainability and drive resources toward unmet needs and evaluation.
Communities should consider the following:
- How can agreement on a few key child and family-focused metrics across sectors be achieved early on?
- What types of TA regarding data collection and evaluation are needed from funders?
- How can early findings be used to inform continuous improvement within the portfolio of interventions to drive changes to improve the health of children and families?
Conclusion
Optimizing health across the lifespan requires greater investment in children and families by transforming community systems to focus on prevention and wellbeing. The priorities and approaches summarized here represent the wisdom and practices of many health, research, philanthropy, and community leaders across the country who contributed emerging ideas, insights, and findings. These priorities and approaches are offered to catalyze further testing of ACHCF models and advance adoption of innovative and effective approaches that have the potential to improve health and well-being for children and families over the long term.
Join the conversation!
![]() Tweet this! Child growth, development, and well-being are impacted by the communities in which children live, including systems that care for them, like schools. Read about how a community-based approach can support children and families: https://doi.org/10.31478/202001b #NAMPerspectives
Tweet this! Child growth, development, and well-being are impacted by the communities in which children live, including systems that care for them, like schools. Read about how a community-based approach can support children and families: https://doi.org/10.31478/202001b #NAMPerspectives
![]() Tweet this! Decades of research points to the importance of collaborating with communities to address the drivers of health outcomes. This #NAMPerspectives outlines how an Accountable Communities for Health approach can promote the health of families: https://doi.org/10.31478/202001b
Tweet this! Decades of research points to the importance of collaborating with communities to address the drivers of health outcomes. This #NAMPerspectives outlines how an Accountable Communities for Health approach can promote the health of families: https://doi.org/10.31478/202001b
![]() Tweet this! Optimizing health across the lifespan requires greater investment in children and families by transforming community systems to focus on prevention and well-being. This #NAMPerspectives outlines a potential model: https://doi.org/10.31478/202001b #NAMPerspectives
Tweet this! Optimizing health across the lifespan requires greater investment in children and families by transforming community systems to focus on prevention and well-being. This #NAMPerspectives outlines a potential model: https://doi.org/10.31478/202001b #NAMPerspectives
Download the graphics below and share them on social media!

References
- WHO (World Health Organization). 2008. Children are not little adults. Available at: https://www.who.int/ceh/capacity/Children_are_not_little_adults.pdf (accessed December 9, 2019).
- Shonkoff, J. P., W. T. Boyce, and B. S. McEwen. 2009. Neuroscience, molecular biology, and the childhood roots of health disparities: Building a new framework for health promotion and disease prevention. JAMA 301(21):2252–2259. https://doi.org/10.1001/jama.2009.754
- Cassidy, A. 2011. Health policy brief: Community development and health. Health Affairs. https://doi.org/10.1377/hpb20111110.912687
- Jutte, D. P., J. L. Miller, and D. J. Erickson. 2015. Neighborhood adversity, child health, and the role of community development. Pediatrics 135(S2):S48. https://doi.org/10.1542/peds.2014-3549F
- Braunstein, S., and R. Lavizzo-Mourey. 2011. How the health and community development sectors are combining forces to improve health and well-being. Health Affairs 30(11). https://doi.org/10.1377/hlthaff .2011.0838
- George Washington University School of Public Health. 2019. Funders Forum on Accountable Health. Available at: http://accountablehealth.gwu.edu (accessed December 9, 2019).
- Mongeon, M., J. Levi, and J. Heinrich. 2017. Elements of accountable communities for health: A review of the literature. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201711a
- ASCEND The Aspen Institute. n.d. Guiding principles. Available at: http://ascend.aspeninstitute.org/two-generation/guiding-principles (accessed December 9, 2019).
- Milstein, B. 2018. No more fragmentation: Crafting a comprehensive strategy for regional health and well-being. The ReThinkers’ Blog. Available at: https://www.rethinkhealth.org/the-rethinkers-blog/no-more-fragmentation-crafting-a-comprehensive-strategy-for-regional-health-and-well-being (accessed December 9, 2019).
- NRC and IOM. 2000. From neurons to neighborhoods: The science of early childhood development. Washington, DC: National Academy Press. https://doi.org/10.17226/9824
- NASEM (National Academies of Sciences, Engineering, and Medicine). 2019. A roadmap to reducing child poverty. Washington, DC: The National Academies Press. https://doi.org/10.17226/25246
- Gratale, D., and D. Chang. 2017. Defining an accountable community for health for children and families. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201710e
- Harvard University Center on the Developing Child. 2010. The foundations of lifelong health are built in early childhood. Available at: https://developingchild.harvard.edu/wp-content/uploads/2010/05/Foundationsof-Lifelong-Health.pdf (accessed December 9, 2019).
- Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine 14(4):245–258. https://doi.org/10.1016/S0749-3797(98)00017-8
- Hughes, K., M. A. Bellis, K. A. Hardcastle, D. Sethi, A. Butchart, C. Mikton, L. Jones, and M. P. Dunne. 2017. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2(8):e356–e366. https://doi.org/10.1016/S2468-2667(17)30118-4
- Monk, C., W. P. Fifer, M. M. Myers, R. P. Sloan, L. Trien, and A. Hurtado. 2000. Maternal stress responses and anxiety during pregnancy: Effects on fetal heart rates. Developmental Psychobiology 36(1):67–77. Available at: https://pubmed.ncbi.nlm.nih.gov/10607362/ (accessed September 2, 2020).
- Shonkoff, J. P. 2016. Capitalizing on advances in science to reduce the health consequences of early childhood adversity. JAMA Pediatrics 170(10):1003–1007. https://doi.org/10.1001/jamapediatrics.2016.1559
- Cornell Project 2 Gen. 2019. What is 2Gen? Available at: http://www.2gen.bctr.cornell.edu/what-is-2gen-1 (accessed December 9, 2019).
- ASCEND The Aspen Institute. 2016. Two-generation playbook. Available at: https://ascend.aspeninstitute.org/wpcontent/uploads/2017/10/Playbook_Sept_2016.pdf (accessed December 9, 2019).
- IOM and NRC (Institute of Medicine and National Research Council). 2014. Strategies for scaling effective family-focused preventive interventions to promote children’s cognitive, affective, and behavioral health: Workshop summary. Washington, DC: The National Academies Press. https://doi.org/10.17226/18808
- Perrin, E. C., L. K. Leslie, and T. Boat. 2016. Parenting as primary prevention. JAMA Pediatrics 170(7):637–638. https://doi.org/10.1001/jamapediatrics.2016.0225
- Colorado Department of Human Services. 2019. The two-generation (2gen) approach. Available at: https://www.colorado.gov/pacific/cdhs/two-generation-approach (accessed December 9, 2019).
- Bell, J., and V. Rubin. 2007. Why place matters: Building a movement for healthy communities. PolicyLink. Available at: https://www.policylink.org/sites/default/fi les/WHYPLACEMATTERS_FINAL.PDF (accessed December 9, 2019).
- Donnelly, L., I. Garfinkel, J. Brooks-Gunn, B. Wagner, S. James, and S. McLanahan. 2017. Geography of intergenerational mobility and child development. Proceedings of the National Academy of Sciences 114(35):9320–9235. https://doi.org/10.1073/pnas.1700945114
- Build Initiative. 2019. High-poverty neighborhoods. Available at: https://www.buildinitiative.org/Resources/50-State-Chart-Book/17-High-Poverty-Neighborhoods (accessed September 2, 2020).
- Beck, A., E. Edwards, J. Horbar, E. Howell, M. McCormick, and D. Pursley. 2019. The color of health: how racism, segregation, and inequality affect the health and well-being of preterm infants and their families. Pediatric Research. https://doi.org/10.1038/s41390-019-0513-6
- NASEM. 2019. Vibrant and healthy kids: Aligning science, practice, and policy to advance health equity. Washington, DC: The National Academies Press. https://doi.org/10.17226/25466
- Mauri, A., J. Unützer, R. Ferguson, H. Harbin, A. Carlo, and M. Schoenbaum. 2017. Payment reform and opportunities for behavioral health: Alternative payment model examples. Available at: https://chp-wp-uploads. s3.amazonaws.com/www.thekennedyforum.org/uploads/2017/09/Payment-Reform-and-Opportunities-for-Behavioral-Health-Alternative-Payment-Model-Examples-Final.pdf (accessed December 9, 2019).
- New York State of Opportunity Department of Health. 2017. Value-based payment for children. Available at: https://www.health.ny.gov/health_care/medicaid/redesign/dsrip/vbp_library/docs/2017-09-12_child_cag.pdf (accessed December 9, 2019).
- Vital Village. 2019. Community of Practice. Available at: https://www.vitalvillage.org/system-change (accessed September 2, 2020).
- Chao, R., S. Bertonaschi, and J. Gazmararian. 2014. Healthy beginnings: A system of care for children in Atlanta. Health Affairs (Millwood) 33(12):2260–2264. https://doi.org/10.1377/hlthaff .2014.0706
- Hester, J. 2018. A balanced portfolio model for improving health: Concept and Vermont’s experience. Health Affairs 37(4):570–578. https://doi.org/10.1377/hlthaff .2017.1237
- Center on the Developing Child at Harvard University. 2017. Three principles to improve outcomes for children and families. Available at: https://developingchild.harvard.edu/resources/three-early-childhood-development-principles-improve-child-family-outcomes (accessed December 9, 2019).
- Washington State Institute for Public Policy. 2018. Benefit-cost results. Available at: http://www.wsipp.wa.gov/BenefitCost (accessed September 2, 2020).
- Cantor, J., R. Tobey, K. Houston, and E. Greenberg. 2015. Accountable communities for health: Strategies for financial sustainability. JSI Research & Training Institute, Inc. Available at: http://www.communitypartners.org/sites/default/fi les/documents/cachi/resources/JSI%20ACH_Sustainability_Final_2015_05.pdf (accessed December 9, 2019).
- Cabello, M., and K. Ballard. 2018. Braiding and blending: Managing multiple funds to improve health. PFS Perspectives. Available at: https://pfs.urban.org/pay-success/pfs-perspectives/braiding-and-blending-managing-multiple-funds-improve-health (accessed December 9, 2019).
- Counts, N. Z., N. Halfon, K. J. Kelleher, J. D. Hawkins, L. K. Leslie, T. F. Boat, M. A. McCabe, W. R. Beardslee, J. Szapocznik, and C. H. Brown. 2018. Redesigning provider payments to reduce long-term costs by promoting healthy development. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201804b
- Chang, D. I., and L. Simpson. 2018. Spurring innovation: The role of child health policy. Moving Health Care Upstream. Available at: https://www.movinghealthcareupstream.org/spurring-innovation-the-role-of-childhealth-policy (accessed December 9, 2019).
- Johnson, K., and C. Bruner. 2018. A sourcebook on Medicaid’s role in early childhood: Advancing high performing medical homes and improving lifelong health. Child & Family Policy Center. Available at: https://www.cfpciowa.org/documents/fi lelibrary/medicaid_finance/section_pdfs/Combined_piece_5A8095C6D6B29.pdf (accessed December 9, 2019).
- Hagan, J. F., J. S. Shaw, and P. M. Duncan. 2017. Bright futures: Guidelines for health supervision of infants, children, and adolescents. Fourth Edition. Elk Grove Village, IL: American Academy of Pediatrics. Available at: https://brightfutures.aap.org/Bright%20Futures%20Documents/BF4_Introduction.pdf (accessed December 9, 2019).
- New York State Department of Health. 2019. First 1000 days on Medicaid initiative. Available at: https://www.health.ny.gov/health_care/medicaid/redesignfi rst_1000.htm (accessed December 9, 2019).
- Boots, S. W. 2015. New ways of creating opportunities for families in poverty: Perspective on the emerging two-generation policy discussion. First Focus on Children. Available at: https://firstfocus.org/resources/report/new-ways-of-creating-opportunities-forfamilies-in-poverty-perspective-on-the-emergingtwo-generation-policy-discussion (accessed December 9, 2019).
- Data Across Sectors for Health. 2019. About DASH. Available at: https://dashconnect.org (accessed December 9, 2019).
- Nemours Children’s Health System. 2018. Community care coordination systems: Technology supports. Available at: http://www.movinghealthcareupstream.org/wpcontent/uploads/2018/09/FINAL_Nemours_CommCareSysTechSupp.pdf (accessed December 9, 2019).
- Hewitt, A., D. Gratale, N. Counts, L. Hogan, and D. Chang. 2019. Data sharing across child-serving sectors: Key lessons and resources. Available at: https://www.nemours.org/content/dam/nemours/wwwv2/fi lebox/about/data-sharing-brief.pdf (accessed December 9, 2019).