Patients and Health Care Teams Forging Effective Partnerships
Introduction
“Will I do better if my care is delivered by a team? Will my chance of having a better outcome improve? This is what I value. This is the bottom line.”
Jessie Gruman (1953-2014), founder and president of Center for Advancing Health and workgroup member.
In a discussion paper published by the Institute of Medicine (IOM) in 2012, the authors laid out the core principles and values of effective team-based health care in the belief that achieving a three-part aim—improving patients’ experience of care, achieving better population health, and reducing per-capita cost of health care—would require clinicians to work effectively in teams and for multiple teams to work effectively with each other (IHI, 2014; Mitchell et al., 2012). They also underscored that the promise of high-value and high-quality health care could not be realized without including patients (Please note that any reference to “patient” throughout this paper includes the patient and his/her family, with “family” referring to anyone who functions in that capacity on behalf of the patient, such as a caregiver.) and their families as invited members of, or partners with, their health care teams (Wynia et al., 2012).)
In this discussion paper, we explore how patients view their role in team-based care and explain what is needed to foster effective partnerships of patients and health care providers to create high-functioning teams that meet patients’ needs. It stems from the view that it is important that the evolving health care system better serve patients and society and that team-based care and effective partnerships with patients across the care continuum contribute to achieving that goal. Team care takes place in various settings and clinical situations, and because it is beyond the scope of this work to explore all of these diverse settings, we focus on primary care settings where team-based care is provided.
The authors (Suggested citation: Okun, S., S. Schoenbaum, D. Andrews, P. Chidambaran, V. Chollette, J. Gruman, S. Leal, B. Lown, P. Mitchell, C. Parry, W. Prins, R. Ricciardi, M. Simon, R. Stock, D. Strasser, C. E. Webb, M. Wynia, and D. Henderson. 2014. Patients and Health Care Teams Forging Effective Partnerships. Discussion Paper, Institute of Medicine, Washington, DC. http://nam.edu/wp-content/uploads/2015/06/patientsForgingeffectivePartnerships) are participants drawn from the Best Practices Innovation Collaborative of the IOM Roundtable on Value & Science-Driven Health Care, which seeks to improve public understanding, appreciation, and evidence-based discussion of the nature and use of evidence to guide clinical choices. The Collaborative is inclusive and its participants are drawn from organizations representing clinicians on the front lines of health care delivery, employees of government agencies either actively involved in patient care or with programs and policies centrally concerned with identification and application of best clinical services, members of the health professions, patients and patient advocates, and others involved in transforming health care.
We offer background about patient-centered care in the United States and team-based care. We then present general findings, including rich details derived from the literature review and one-on-one interviews, which appear in the appendix. The interviews extend our past work and differentiate this paper from its predecessor. In interviewing patients, surrogate decision makers, providers who practice team-based care, and organizations that champion such care, we found a common thread: The desire for clear roles for patients on their health care team, shared decisions, and enhanced communication between patients and other health team partners.
We begin by highlighting key takeaways identified from the review and interviews, and conclude with targeted suggestions for practice- and organization-based improvements as well as ideas for the research community to broaden the knowledge, understanding, and evidence base for effective patient-centric partnerships in team-based care across the full continuum of settings and time.
Key tenets for partnering with patients on health care teams
- Ensure clarity about patients’ roles as health team partners. Patients and providers want clarity about roles and expectations for patients as team members that recognize variation from one patient to another as well as team-to-team variation. Patients want care that is coordinated and considers their real life as a whole person, not just as a patient defined by a health condition. In some cases, providers may simply meet patients where they are because some patients already seek to play more active roles in their care, but are unclear how to proceed. In some cases, providers may need to be more proactive and invite, facilitate, and nurture such active partnerships with patients. (See Table 2, p. 11.)
- Support shared and personalized decision making. Providers should be consistent and proactive in inviting patients to partner and should welcome the dynamic nature of patients’ preferences for participating in care and shared decision making. Patients may prefer a more passive role some or even all of the time; providers need to anticipate and respect that. Readiness of key stakeholders to support creative and collaborative partnerships is essential for effective high-functioning teams.
- Enhance communication among care team partners. Patients and providers want effective communication channels that support transparency and availability of health care information (e.g., lab results) and patients want convenient access to information and the team (e.g., portals, e-mail, a single point person). Research should seek out patients’ perspectives and insights about vocabulary, roles, and expectations and should collect data on outcomes and experiences of care, both positive and negative.

There are unprecedented opportunities to reimagine health and health care through effective partnerships supported by the evolving culture of patient-centered engagement and empowerment, together with advances in health information technology, patient-generated health data, and health-monitoring devices. All of the partners—the patient, his or her family, his or her clinicians, and others—have meaningful roles to play. Each brings something unique and important to the relationship (see Table 1).
Each patient’s role on the health team should reflect their preferences, their values, and their desired outcomes. This is, after all, the bottom line.
The current state
The notion of patient-centered care is continuously evolving as more is learned about the potential impact, and as new approaches are developed. In the mid-2000s, the National Committee for Quality Assurance (NCQA) developed a process for recognizing primary care practices as patient-centered medical homes (PCMHs). By 2014, nearly 7,000 U.S. primary care practices—more than 10 percent—had been recognized as PCMHs, distinguishing themselves by meeting a number of requirements and aiming to attune care delivery closely to patients’ health care wants and needs (NCQA, 2014). The 2014 revised standards for NCQA recognition emphasize collaborating with patients as part of the care team and establish team-based care as a “must-pass” criterion. Similarly, in the National Patient Safety Foundation’s “Universal Patient Compact,” reaffirmed in 2011, health care practitioners’ first pledge is to include patients “as a member of the team,” and patients’ first pledge is to be “a responsible and active member” of the health care team (National Patient Safety Foundation, 2011).
When patients and family caregivers are fully involved in care decisions and health care practices, the results are better, readmission rates and risk of suffering an adverse event can decline, patients’ satisfaction rating of their experience can rise, and costs can drop (Anderson, 2007; Boulding et al., 2011; Weingart et al., 2011; Hibbard et al., 2013; James, 2013; Hibbard and Gilburt, 2014). Accordingly, it is important to identify and disseminate best practices for inviting patients to become active partners with their health care teams to the degree they desire and are able. This calls for ongoing collaboration of health care teams with patients and family caregivers to ensure that they are comfortable with candid interactions with health professionals and providing feedback that strengthens the relationship and their mutual understanding of the patient’s needs and how they may best be addressed.
Strong primary care, the care setting focused on in this paper, is critical to achieving better patient outcomes, especially as the prevalence of multiple chronic health conditions increases (AHRQ, 2014a). More than 75 percent of U.S. health care spending is devoted to treating persons with chronic conditions (CDC, 2009). Of course, specialists and subspecialists also play very important roles. The complexity of care and services often required today requires health professionals across the system to work with people in a coordinated, collaborative way and to consider the whole person—not just the condition or array of conditions that a person might have (Bodenheimer et al., 2002).
All patients bring unique expertise regarding their preferences, skills, knowledge, and experiences into a potential relationship with a health care team. Patients—and, often, their families and caregivers—live with their conditions and symptoms 24 hours a day, 7 days a week. Patients are experts in knowing how they feel from moment to moment and day to day. However, not all patients are well informed about their medical conditions and how best to manage them (Fagerlin et al., 2010). Relatively few come to medical encounters with the same technical skills, clinical knowledge, and detailed understanding of the health care system that most clinicians have. Some patients prefer to be involved at a more detailed level, others less so (Alston et al., 2012). But many patients and family members have acquired, and many more are capable of developing, considerable knowledge, skills, and confidence in decision making that could influence their outcomes positively—especially those outcomes that matter most to them.
Only recently, with increased attention on patient-centered care at the practice level, has it become evident that a large percentage of patients who have personal physicians and, especially minorities, do not have an effective health care team (Beal et al., 2007). When people have a personal physician and an effective practice team, their outcomes are better (Beal et al., 2007; Havyer et al., 2014).
There is still much to learn about the practical realities of patients becoming true partners in their care, and the most effective teachers will be patients themselves. When patients and clinicians have an effective partnership, the relationship becomes more fluid. It transcends the traditional roles of learner and teacher, leader and follower. Valid, ongoing assessments of team functioning and performance, including assessments by patients themselves, will be important to identify and illuminate team functioning and the strength of the partnership with patients, and to inform improvement efforts so that demonstrably better patient outcomes can be achieved consistently.
Methods
Given the scope of the project, an early decision of the authors was to divide our work into three informal activity streams, each with a specific focus—literature review, patients’ insights, and clinicians’ and organizational insights. In the course of the work, discussions have been conducted through the IOM Best Practices Innovation Collaborative meetings, May 2013 and March 2014, which have provided helpful guidance and suggestions to us that were incorporated into writing this paper.
Our literature and science knowledge stream participants gleaned what is known from published literature about patient involvement in health care teams and identified what remains unknown. The current knowledge activity stream participants selected interview questions and conducted semistructured, one-on-one interviews with clinicians and with leaders of organizations that champion fostering patient engagement. The data collection knowledge stream participants designed an interview guide and contracted for semi-structured interviews to occur with patients and surrogate decision-makers to gather their unique perspectives and insights about team-based health care and patients’ participation on the team. Details about each activity stream follow.
Insights from the Literature Review
In 2013, a comprehensive review was conducted of PubMed, Sociological Abstracts, and PsycInfo for journal articles published from 2005 to 2013 that related primarily to health care teams providing patient-centered care for chronic conditions across the lifespan.
For literature and science, five broad inquiries were identified with sweeping road map questions related to health care teams to inform the review process. The road map questions focused on existing typologies for health care teams, basic knowledge about what makes teams work, potential roles for patients on the team, philosophical or ethical considerations of interest, and possible impact of integrating patients as partners with their health care team. (See Appendix B for the questions that informed the search and for a summary of the literature review.) The literature search was conducted by staff of the Agency for Healthcare Research and Quality (AHRQ).
Findings from the literature review and an environmental scan suggest that high-functioning health care teams are characterized by the strength of relationships, processes, interactions among the individuals who form the team, and goal-directed activities (Shoemaker et al., 2013, unpublished). Effective health care teams include a mix of people, talents, and capabilities that perform interdependent functions to fulfill the needs of patients with whom they partner. (See Questions and Answers that are interspersed throughout this paper.)
There are many types of teams in health care. A team can be as small as a single health care provider, and a patient or a team can include others who support that patient’s care, including people who are outside of the health care organization or institution (Dyer, 1984; Salas et al., 1992).
In addition to the core values and principles of team-based care identified in the 2012 discussion paper, the literature revealed a number of ways to describe conditions deemed necessary to promote team members’ engagement, including patients and high functioning by teams (Mitchell et al., 2012). Building blocks for effective team-based care include focusing on respectful interaction; rich communication; mindfulness; trust; continuous learning; and shared, explicit goals and accountability. Importantly, many papers describe the presence of dynamic, participatory leadership as a catalyst across all domains of high-functioning health care teams.
Patients’ roles on health care teams can evolve and patients can interact with a number of teams as they move through the trajectory of care, as they age, or even during a single treatment. The patient is the common thread and the person who most needs to benefit from his or her interaction with these teams (see Table B-1, pp. 44-46). Just as practitioners need training in how to foster a clinical environment that is conducive to involving patients in care decisions, patients and caregivers also need instruction in how to define outcomes that matter most to them in order to align care with their individual capabilities, preferences, and values.
In our review of 65 abstracts about team-based care, we found that patients’ roles on the health care team were typically implicit and were rarely described in detail—despite the central importance of patients in the work of teams. Examples in which patients’ roles were described in more detail included research describing patients’ participation in group education programs, patients expressing their values and preferences for end-of-life care in team meetings, self-management, knowledge sharing, collaborating with the health care team as an improvement partner, participation in bedside reporting during shift changes, planning and evaluation of services, participation in care planning, understanding and using tools to monitor health (e.g., pedometer, glucose monitoring, and blood pressure monitoring), and setting and endorsing treatment goals. Participation in shared decision making (SDM) was cited most frequently as a key role for patients and families on the team (see Table B-2, pp. 49-53).
In sum, there is much to learn from the literature about team-based health care, but only a few dozen papers specifically address the role of patients as members of or partners with clinical teams. Although many practice settings are interested in engaging patients in their care, the literature describes relatively few settings with a process to include patients and their families as active participants in the care team. Most of these are related to managing chronic conditions, such as diabetes and hypertension. Much of the relevant literature on patients’ roles on health care teams is framed around their roles in SDM, though numerous efforts are underway to engage patients in all aspects of health and health care. Recent patient engagement efforts include involving patients in quality improvement projects, helping to design new care delivery models, and serving as members of patient and family advisory councils. Federally Qualified Health Centers (FQHCs) seek to ensure patient engagement through governance and require that 51 percent of the FQHC board comprise members of the patient population served by that health center.
The literature review also revealed that the vocabulary to describe patient involvement in team-based care is in flux. Do patients prefer to be described as “engaged” in their health and health care? Do they want to be a team “member”? Or, does the notion of “partner in care” resonate better? What do these terms mean in relation to issues of team communication and patterns of decision making? For the purposes of this paper, we developed brief descriptions of how various patient roles in relation to health care teams could be linked to ways of thinking about communication, information flow, and different models of clinical decision making (see Table 2, p. 11). We believe these questions about how best to describe patients’ roles on teams—a continuum that spans from “care to me,” “care with me,” and “care by me”—and many more should be posed to patients themselves to answer as they become more familiar with team-based models of care.

Insights from Patients
Our second activity stream participants transformed the broad questions that guided the literature review into a shorter list of questions with follow-up probes that were used in semi-structured, one-on-one telephone interviews with 15 patients and their proxies to understand their perspectives about team-based care. The interview guide was refined through pilot testing and further revised after consultation with and approval by the Committee to Review Human Subjects, acting as The National Academies’ Institutional Review Board. Outreach was made to NCQA Level 3-rated patient-centered medical homes located across the country. (Outreach was made to facilities located in California, Colorado, Georgia, Iowa, Maryland, Massachusetts, Michigan, New York, North Carolina, Ohio, Pennsylvania, South Carolina, and Washington state. Additional outreach was made via safety net facilities and organizations based in California, Massachusetts, Texas, and Washington, DC.) NCQA-rated practice settings were selected because we sought to understand team-based care from patients’ experiences within settings delivering team-based care. An initial group of 10 people who experienced team-based care was interviewed from November 20 to December 13, 2013. The interviewees ranged in age from 37 to 86 and were living with a myriad of health conditions, including minor illnesses, chronic conditions, and various other ailments. Two interviewees were 45- and 52-year-old caregivers who described their views of team care their children received. (See Table 3 on p. 12 for patients’ and caregivers’ demographics.)
Data from the first 10 interviews were reviewed to inform the patient mix for the final five interviews. The data collection volunteers were provided access to individual transcripts and reviewed a high-level thematic summary. They used these analyses to make minor modifications to interview guide questions in order to elicit granular detail from subsequent interviewees. (See Appendix C on p. 66 for the interview guide questions and probes and view full transcripts of the patients’ interviews here.
Review of the first 10 interviews revealed that interviewees had an unusually high degree of sophistication and knowledge of the health care system, with atypical levels of activation and, in some cases, professional health care experience. One interviewee, a former nurse, reported using a home blood pressure “cuff” to compare her readings with those acquired in the clinician’s office to prove that her blood pressure readings were elevated by the stress of office visits, rather than a chronic condition that would require medication. Another pushed to the highest level at his former place of employment, a health-related firm, to access care from one of the nation’s leading specialists. Two other interviewees, identified as patient “partners,” work with their primary care practice on quality improvement efforts.

In pre-interview conversations with these two patients, the interviewer asked that they answer questions from their personal perspective as patients.
We established exclusion criteria for the second group of five interviews in order to identify patients who would be more representative of the general population. These patients were selected to enhance patient diversity by age, ethnicity, race, and degree of prior involvement in health care. Five additional patients, aged 37 to 67 years, were interviewed via telephone by the external consultant from February 25 to May 19, 2014.
The interviews offer insights into how patients view team-based care, what works, and what doesn’t. The patients’ stories illuminate the fact that these patients want providers to be deliberate, or proactive, about transparency and shared decision making. The patients we interviewed want to feel they are listened to by their providers, cared for and about, and invited to participate to the extent they desire.
The one-on-one interviews explicitly sought patient’s and caregiver’s perspectives about a patient’s role on the team and, more specifically, the patient’s own personal role on their health care team. The results of the interviews are organized in five thematic categories:
- Defining team-based care with clarity about roles and expectations;
- Partnership in decision making about treatments and care;
- Patient proactivity and personalized responsibilities;
- Coordinated care that considers the patient as a whole person; and
- Communication that is personalized and convenient.
These are discussed below with illustrative direct quotes from patients and family caregivers.
Theme—Defining team-based care

Several patients described a rationale for team-based care and valued the synergy and knowledge that can come from many clinicians with varied training and viewpoints contributing to their care. One such patient equated team care with “getting a broader view of my particular condition and a plan for my health” and underscored the value of multiple perspectives: “I feel more eyes and ears looking at me give me a better chance of [getting] good care.” Others noted that their care was more organized and coordinated in a team approach. Despite the degree of sophistication among the first 10 interviewees, however, some patients who were clearly receiving team care remained uncertain about the nature of team care. When a 75-year-old patient who typically saw a specialist during annual visits was, instead, seen by a physician assistant, the unexplained switch sowed confusion and concern.
“I thought, well did my, did the specialist leave? … I felt a little negative about it that, you know, they’re just pushing me around and not telling me why … I should have confidence in this new person that I’m going to be seeing. [They] didn’t explain what her background is. … I didn’t understand that these two people were on the same team and [that] certainly was kind of excluding me from any sense of team.”
When asked to list the members of their health care teams, all participants listed a primary care physician and, in many cases, multiple physicians and/or specialists, depending on the complexity and severity of their illness. In addition to naming physicians, interviewees also listed an ensemble cast made up of a few or many other players, including cardiologists, dentists, gastroenterologists, hematologists, medical assistants, neurologists, nurse practitioners, oncologists, ophthalmologists, physical therapists, physician assistants, receptionists, social workers, surgeons, and other specialists. A few pointed to support staff as team members, with both positive and negative attributes. Some interviewees expressed enthusiasm about the manner in which team members worked together: “They all work together as a team. … [F]rom the minute I walk in the door, it’s everyone on the staff that contributes to my care from the receptionist and the medical assistants to the practitioners. … I feel like there’s a rapport that’s developed from the receptionist on up,” one patient said.
Interviewees commented on the value of specific team member’s contributions, such as the diabetes educator who was able to target lifestyle issues in disease management, or a medical assistant who was helpful in providing free pharmaceutical samples for a patient whose primary source of income was disability checks. Alternately, one interviewee, a patient in her clinic for more than 20 years, identified specific team members as “weak” links and pointed to high turnover in the non-clinical staff as a possible indicator that a team may not be functioning optimally. She said, “I know they’re trying to build a team concept. I am disappointed, and I think there’s a weak link in this whole team in the, what they call the MA (medical assistant)…I do not have confidence in their skills for getting the correct blood pressure—which is a big deal for me. And there’s such, there’s a turnover, and that’s bothersome. Something is not working.”
Theme—Partnership in making decisions

Many interviewees identified themselves as a member of the care team and reported providing direct input on treatment decisions. To most, being a member of the team meant being included in discussions, having a say, and knowing that the team was listening.
A caregiver whose 6-year-old son suffers from multiple health conditions described a series of actions that cemented her role as an active health team member: “No. 1 [is just] having the doctors actually listen and validate your concerns. And then, No. 2, to be able to ask ‘What is best for the family?’ The family’s take on things is just as important as the physician’s. …We’ve been told, ‘You have a couple of different treatment options, but this is going to happen with this and these other side effects are going to happen with this. Which way do you want to go?’ ”
Interviewees expressed varied levels of interest in engaging in decision making. One group of patients noted the importance of having their concerns validated and their input elicited, as well as being given choices and evidence to inform their choices. In the words of one such patient, “I have full say. My voice is respected. My questions are answered. I’m given time to raise whatever issues may come up, and I feel I’m really being heard.”
A 53-year-old man who underwent complicated surgery followed by lengthy rehabilitation added that he and his wife make a list of questions in advance. “[W]e don’t let the doctors leave our room till we answer all our questions,” the man said.
By contrast, a subset of patients wanted to be treated with respect and have their questions answered, but did not want to be active team members; some preferred to delegate authority to their providers. One interviewee, a 67-year-old woman, expressed concerns about patients’ competency to participate in decision making and noted that team care could be viewed as a negative development if “all the decisions were left on the patient.” What these interviews highlight is not just variability in the perception and experience of patients being team members, but also in patients’ desire for and ability to actively engage in decision making, a theme that is expanded on in the next thematic category.
Theme—Patient proactivity and responsibility

Many patients fully embraced the idea of being active participants in their health care and rejected the notion of being “passive.”
“I think, as a patient, you need to be very proactive about your care. … You know the doctors can only make decisions and make prognostications based on the information they get and the best source of that information is you, the patient. So, I think patients all have to do this and, in fact, it is perhaps one of the most important things that a patient can do to tip the cards in their favor to really extend your life,” one patient said.
Admittedly, patient proactivity may create tension when patient and provider opinions diverge. A 53-year-old man whose treatment choice differed from the option preferred by his team of clinicians elaborated: “I could see their frustration. … I told them how I was going to proceed, what I was willing to accept for treatment. [The] doctors weren’t happy, but I forced them to follow me in that path for the simple reason I wasn’t going to do what they wanted me to do.”
Several interviewees, however, acknowledged that some patients would not relish playing a more active role in their health care or lack the capacity to do so. In reflecting on the use of technology to enhance patient engagement, a 67-year-old interviewee commented that patient portals are “fine for people who are computer literate. But for those who aren’t, I feel as though there should be … some way that their care providers can either communicate with them or to them or at least a family member that can explain it to them.”
Finally, a 52-year-old patient with cancer said that while his team quickly let him know that he was “the boss,” and the team works for him, he still valued being able to turn day-to-day decisions about his care over to his oncologist when he was too ill to provide such oversight, echoing a theme raised in the clinicians’ interviews about the relationship between declining health status and patients’ activities as team members.
Theme—Care coordination

Not surprisingly, more frequent users of health care provided the most detailed explanations of how team care could be improved. A 59-year-old patient with cancer described the synchronized actions that are required for multiple appointments to run smoothly, noting the complex sequencing of tests and treatments. If insufficient time is allotted for the blood test at check-in, “the chemo was delayed because they work on a very tight schedule for patients. So, that all has to work like clockwork to be able to stay on track.”
Many patients thought that coordinated care was a “good” thing and envisioned ideal care including a care coordinator who served as “the hub of all of these different spokes.” An illustration of the benefits provided by coordinated care was given by a family caregiver whose 6-year-old son’s hospital uses a scheduling center for children who see multiple clinicians, allowing her to trim extraneous trips to the facility by scheduling lab work, provider appointments, and prescription pick-up on the same day. “Even the dental clinic works in conjunction with the operating room so whenever we’re there and he’s going under general anesthesia for a surgical procedure, they’ll go in and do his dental X-rays and clean his teeth,” the 45-year-old mother said.
Comparing the care they receive and the ideal, however, many found room for improvement in care coordination. A 52-year-old family caregiver described her search for answers typically becoming an odyssey as she called one hospital department after another. “If I could just call one nurse or nurse practitioner and say ‘This is going on, and I’ve had this, I’ve had like a test result come back weird.’ And I didn’t know if it was colorectal. I didn’t know if it was urology. I didn’t know if it was neurosurgery. And so, you know, I called and they’re like, ‘No, we don’t think that’s us. Why don’t you try colorectal?’ I call them, you know. It would be great to have a person that I can say, ‘Look, what’s going on with this test result? Can you find out and get back to me?’ ”
Theme—Communication

An integral component to a well-functioning health care team, according to the patients interviewed, is their ability to communicate with clinicians and for health care practitioners to communicate effectively among themselves. Patients characterized feeling heard and respected, and having a provider who listened, as “good” communication. A 37-year-old man switched primary care clinicians and said he appreciated how his new physician solicits his viewpoint. “[T]he doctor really listens to what’s wrong with you. He don’t just go in there and tell you: ‘This is what is wrong with you.’ He asks, you know, ‘What’s bothering you?’ Then, he does his thing.”
In addition to effective patient–provider communication, interviewees equated team care with effective and transparent communication among providers. Central to a 67-year-old patient’s belief that she receives team care is the knowledge “they’re looking at my record and they have information about me and know about a previous visit and know about, for example, the results: If my cardiologist sends a report to my internist and she’s aware of it. If people are aware of blood results and what medications I’m on and, you know, the latest visit I had with any one of them.”
Alternately, poor communication among providers may erode patients’ confidence in the quality of their care and in the notion their providers function as a team. A 75-year-old man whose wife had been diagnosed with cancer recalled her being seen by an oncologist, a surgeon, a radiologist, and other medical professionals at a facility that prided itself on offering team care. Yet, “there was no evidence, at all, of their conferring. And we fully expected, well, ‘team medicine,’ we’re going to see some evidence [that] these guys are talking to each other and, you know, putting together what’s the best course of treatment for her.” The couple ultimately turned elsewhere, a setting in which multiple specialists included them in a group conversation about the wife’s care and, by doing so, demonstrated team care to this interviewee.
Many patients applauded the advent of digital technology to support their communication with the health team. One 67-year-old patient enthused: “I absolutely love the fact that after I have had blood work or an office visit in a particular office … they will send me an e-mail telling me that my information is available on the patient portal…. I like not having to wait the week for the mail to bring me my results. I like not having to be tethered to a phone for a physician to call me, but, at my leisure, I can look onto the patient portal via the Internet and get my results.”
However, that feeling was not universal. In the second wave of interviews, a 67-year-old patient said that she knew the facility offered patient portals but she was not interested in establishing a page in order to make or change appointments and receive lab results. “I’m too busy, I think,” she said. “I work and I am interacting with my computer all day with work-related matters, and I would just prefer to handle appointments by phone. That’s the easiest thing for me to do and juggle my calendar that way, you know.”
Insights from Clinicians and Organizations
The third activity stream, current knowledge, interviewed clinicians and organizations that are leaders in meaningful patient and family engagement to collect their insights about partnering with patients and families in care teams. The interviewees represented a range of individuals from organizations that included nine provider systems or groups; five organizations that focus, at least in part, on promoting patient engagement, team-based care, or continuous quality improvement; and two employees of a governmental agency. The comments also include viewpoints from health care professionals—a surgeon, a primary care physician, and a nurse—plus two chief medical officers and one chief public health officer. This activity stream was informed by questions that guided the literature review and by the questions that would be posed to patients. The informal subgroup members identified questions best tailored to organizations engaged in this work. The questions were refined through pilot tests; one was deleted due to poor definition and fit. (See Appendix D, p. 68, for the list of organizational members who were interviewed and specific questions that were posed.)
The results of the interviews are organized into four thematic categories:
- Defining team-based care with clarity about roles and expectations;
- Partnership in making treatment decisions;
- Communication methods that support, not inhibit relationships; and
- Organizational and professional challenges.
Theme—Defining team-based care
When asked a similar set of questions, most clinicians we interviewed reported efforts to include patients as members of the health care team and noted that effective two-way communications are at the heart of patient engagement. What’s more, they often said that all parties—patients, family caregivers, and health care professionals—should communicate and coordinate with other members of the team, facilitating understanding, agreement, and coordination of treatment plans, goals, and expectations.
While some interviewees advocated for patients to view themselves as members of their care team and to be active and assertive by, for example, posing questions and ensuring that they understand their treatment plan, others argued for the patient’s role to be fluid and situational—matching their personal preferences and available time. Many interviewees noted that patients contribute valuable insights that no other member of the team possesses.
Theme—Partnership in making treatment decisions
A number of interviewees said patients’ ability to provide input is directly related to their overall health. It can be more challenging to engage frail patients, patients in chronic pain, or patients with cognitive impairments that compromise their memory. Healthy patients who visit solely for an annual physical may not recognize team care in action or their own role on the team.
An internist said that he sees patients regularly for chronic illnesses, such as diabetes and congestive heart failure. Those patients “are more likely to be participants in their care and I need their participation more. A lot of what I am trying to do is effect … change, and I can’t do that without their participation. On the other hand, patients who are really overwhelmed with the burden of disease, sometimes, those patients on the other extreme are difficult to engage: Patients who are at the end of life or have serious medical problems that have high levels of specialty care, people who are undergoing chemo for advanced-stage cancer.”
Theme—Communication
Clinicians pointed to the advent of bedside rounds in standardizing information conveyed to patients and providing an opportunity for patients to pose questions.
At one pediatric center, a staffer said that various members of the care team once entered the patient’s room and gave conflicting information. They’ve resolved the dilemma by ensuring that medical teams write the patient’s care plan on the white board after rounds. “Also, we have a space on our newly designed white boards for white board communication to allow space for the families to write their questions or notes,” the pediatric clinical manager said. “Families can get overwhelmed when the team comes in. … [O]ur staff or the patients or families will write it on the board until they get their answers addressed.”
Such enthusiasm about new means of communication between patients and their care teams was tempered with caution that electronic communication should serve to support, not supplant, face-to-face conversations. One clinician was so concerned that technology would loom as a barrier to face-to-face conversations with patients that he delayed installing computers in examination rooms. Now, he uses the computer as a trigger for enhanced communication with patients. “Just earlier this morning, I had a diabetic patient. She’s lost 32 lbs. She’s proud of herself, and I’m proud, too. I have five years of vital signs. With two clicks, I can create a flow sheet … [and] show her weight. It was steady, way up there. In the last nine months, it’s taken a nose dive. She liked seeing that,” the internist said.
Theme—Organizational and professional challenges

A number of interviewees gave a laundry list of potential barriers for incorporating patients on the health care team, including fear of liability and concerns that patients’ confidence in the ability of the team would be eroded if they knew more about its function.
Some clinicians reported that overcoming such barriers requires enlightened leadership at multiple levels of health care systems, organizations, and individual practices, to ensure a mutual understanding of the principles and practices of including patients and families as partners on the team and a shared commitment to this vision. Leadership commitment is reflected, for example, in resource allocation decisions—including how individuals, money, and time are aligned—and in creating a top-to-bottom culture that embraces care quality improvement efforts that include patients and families.
Another interviewee said clinician education is crucial to producing a generation of health care professionals who are ready, willing, and able to invite patients to engage; who encourage their questions; and who embrace shared decision making. Clinicians can feel challenged by patients’ questions and requests, the interviewee said. A different interviewee noted that another organizational barrier can be the volume of conflicting messages that work against the patient feeling like a part of the system—such as “staff” only, “visitors’ ” hours—all relaying the message that families are outsiders.
Discussion and Conclusion
As demonstrated by the literature review, there is a paucity of published research on the roles of patients or surrogate decision makers as members of or partners with health care teams whose membership is mostly professionals. Thus, it is vital at this stage to gather input from both patients and health care professionals to inform future studies. Qualitative research methods, such as those employed in this inquiry, are well suited to elicit key stakeholder perspectives and outline future research areas.
The interviews conducted and analyzed by our external consultant indicate that many patients value effective team-based health care that treats them as whole persons, not cases, conditions, or diseases. These results align with a recent survey supported by the John A. Hartford Foundation that found that older patients—often characterized as “unwilling to change and suspicious of innovation, particularly about their health care”—were overwhelmingly receptive to the idea of patient-centered medical home practices and that the minority surveyed who were experiencing such team care reported beneficial effects (John A. Hartford Foundation, 2014).
Our interviews also indicate that even clinicians whose practices are currently trying to provide team-based care still have a significant amount yet to learn to meet patients’ expectations for team-based care. All members of the health care team should consider their readiness and capacity to engage in effective partnerships at all levels.
We anticipate questions about the validity of the results and conclusions presented in this paper given the methodologies employed, especially in selecting which patients and clinicians to interview. In anticipation of these questions, we acknowledge that our samples were small and potentially skewed. In fact, we purposefully enriched the clinician sample to include those practicing in organizations that intentionally try to establish meaningful patient and family engagement in health care because we believe these characteristics make it more likely that interesting and important conclusions can be drawn from the interviews. The commonalities in their approaches are worth noting by others as they learn from their example. Their deficiencies, as reported by patients we interviewed, are noteworthy and informative.
Similarly, the patients who were interviewed, while from diverse geographical areas and backgrounds, are not representative of all patients. If anything, many are more sophisticated about their health and the health care systems involved in their care than average patients. They also may be more positive about the notion of team-based care and their roles in it than are average patients. However, to the extent they can identify the negatives as well as the positives and can pinpoint what would make their care and partnerships with teams more effective, we believe those are important observations and likely to provide valuable input for health organizations as they decide to establish or enhance their approaches to team-based care and patient relationships with their teams. Our initial sampling thus serves to highlight the importance of this issue and to underscore the need for broader investigation.
While our work raises many questions, we believe it also offers guidance for future work. In Appendix A, we outline target areas for practice improvement, research, and training.
As organizations increasingly adopt team-based care models and seek to partner with patients to achieve better outcomes and improve patient satisfaction, it will be essential to have a collaborative approach to address how practice teams function and partner with patients. There are some places where patients are actively involved in designing practice improvements (Carman et al., 2013; RWJF, 2014). Yet, it remains atypical for patients to partner in the design and improvement of practices and research so that their perspectives and views are voiced and not merely inferred (Han et al., 2013). It will take work and supportive policies to make meaningful progress. If we have planted the seed for considering patient partnership a core component of quality improvement, our efforts will have been successful. More importantly, this change would increase the chances that the most important stakeholder in this effort, the patient, will be more likely to experience the improved health outcomes we all wish for ourselves.
Appendix A
Improvement Strategies and Priorities
The word “partner” is well understood in the context of a business, such as a law firm, or a personal relationship, such as marriage. However, it is less clear in the context of health care. As we note earlier in this paper, all patients possess intimate knowledge about their preferences, values, and the experience of living with their conditions and symptoms. The concept of considering a patient a member of or partner with their health care team is consistent with the well-accepted precepts of patient-centered care, especially in team-based care (TBC) settings. Yet, as evidenced by the findings in this discussion paper, there is room to improve existing efforts to partner with patients. The time is now for all key stakeholders, including patients, families, practice staff, and organizational leaders, to begin these improvements. In addition, there is much to learn about operationalizing and assessing partnerships in real-world practice, and this necessitates developing an evidence base of research to guide practices and policy makers.
Dissemination of documented improvements in existing practices and the results of research should facilitate the widespread expansion of both team-based practice and partnerships among health care professionals, patients, and families.
Although our list focuses on practice-level activities, it does not end there. Core to achieving these true partnerships is a level of involvement and commitment of patients, staff, and institutional leadership.
We hope that the targets listed below, while not exhaustive, will provide ideas for immediate practice improvements and longer term research opportunities that focus on what effective partnerships of patients and health care teams look like, how they can be emulated, what role creative leadership has on success, and how effective partnerships can demonstrate their effectiveness through evidence of better health and improved outcomes for patients.

Potential practice improvement strategies and research opportunities
Target: Achieve clarity about roles and expectations of patients and families in team-based care
A. Practice improvements:
Health care practices that currently provide TBC can continue the conversations started in this discussion paper by seeking input from patients, families, practice staff, and organizational leaders. Potential activities include:
- Conducting a baseline assessment of perspectives on TBC and patients as partners with or members of the team.
- Identifying key characteristics and actions associated with TBC partnerships.
- Clarifying patients’ and families’ roles on the team irrespective of the specific care setting (e.g., primary care, specialty care, home care, hospice, rehabilitation).
- Describing and routinely sharing information about the roles and expectations of each member of the team across the practice.
- Developing ongoing processes to assess patients’ and family caregivers’ understanding and satisfaction with their roles and responsibilities on the health care team.
Practices considering implementation of TBC can invite all health team partners to provide input and perspectives on how TBC will be defined within the practice and to ensure that roles and expectations of all stakeholders are considered in the context of the practice setting and type by:
- Identifying the range of patient and family roles and developing materials to promote and support effective use of those roles.
- Identifying best practices for identifying and honoring patient and family preferences for their role in partnerships with the health care team that are sensitive and responsive to change.
- Developing marketing materials and community-oriented traditional and social media campaigns that describe, explain, and demonstrate their commitment to effective partnerships with patients and families.
B. Research opportunities:
- Conducting and widely disseminating qualitative research similar to that done by the authors across TBC practices, but on a much wider scale, to elaborate on the essential characteristics of teams that include patients and family caregivers.
- Performing a random sampling of providers and patients in TBC practices to determine the degree to which providers and patients perceive having effective partnerships and the characteristics of each group that are associated with having effective partnerships.
- Exploring the degree of concordance between individual provider’s and patient’s perceptions of effective partnership with specific attention to roles and expectations. Projects should be varied by geographic location, including urban and rural settings, and demographics, such as race, ethnicity, and high and low socioeconomic status.
- Formally evaluating various training methods for forging effective partnerships of patients and health care teams.
- Identifying patient roles and developing materials to support patients in their roles as partners.
- Examining formally the ways to present the concept of partnership with their practices to patients and families.
- Pilot-testing community campaign messaging to introduce the concept of partnership to patients and families.
- Employing measures that are sensitive and specific enough to determine whether the proposed practice improvements achieved the desired aims, such as streamlining care processes, reducing costs, and improving health outcomes.
Target: Measure readiness for and engagement in effective TBC partnerships
A. Practice improvements:
Practices can measure progress toward effective patient partnerships and examine the characteristics of patients within the same health care practice who do and do not seem to have effective partnerships. Potential activities include:
- Assessing the degree to which the practice and the patients feel ready to engage with each other as partners in care management (provider and self-care) and shared decision making.
- Determining whether leadership and the culture of health care systems are ready for patients to partner effectively with health care teams and willing to provide the necessary resources.
- Evaluating all health care team members’ readiness and capacity to participate in shared decision making about treatment and health goals.
- Measuring individual progress toward and satisfaction with outcomes related to mutually agreed-upon health goals using both clinical markers and patient-reported outcome measures.
- Setting and tracking practice-level targets for effective TBC partnerships and transparently reporting on progress toward these targets with all key stakeholders with a specified regularity.
Practices can assess the level of engagement of their staff and patients in effective TBC partnerships and share the results across the organization, including the Patient and Family Advisory Council, where applicable.
B. Research opportunities:
- Formally assessing the characteristics of patients and families who do and do not seem to have effective partnerships with providers, as well as identifying the characteristics of providers in health care practices that, on average, develop more effective partnerships with patients.
- Performing a random sampling of providers and patients in TBC practices to determine the degree to which providers and patients perceive having effective partnerships and the characteristics of each group that are associated with having effective partnerships.
- Developing and formally testing a self-reported metric for use by key stakeholders to measure readiness to engage in effective partnerships across practices and settings.
- Formally testing a set of patient-reported measures that allow patients and family caregivers to measure the effectiveness of partnership with the team on outcomes that align with patients’ preferences and values across practices and settings, including standard quality and safety measures.
- Determining the degree of buy-in at the leadership level at individual practices and the influence of leadership support on the success, failure, and duration of partnering with patients.
Target: Personalize communication, coordination, and decision-making strategies
A. Practice improvements:
- Developing use-cases and protocols for members of the health care team to proactively invite patients and families to engage in partnership.
- Regularly assessing the usability and transparency of TBC practices to support effective partnerships, such as:
- Hours of operation, including after-hours access.
- Availability of a team point person and a process to communicate if the person changes over time.
- Offering options for patients to choose their preference for pre- and post-visit communication, such as e-mail, text message, fax, personal health record, and social media.
- Publicize valid and meaningful performance measures.
- Developing methods for patients and families to personalize their care coordination to reflect “whole person” care.
- Discussing how existing or future patient-generated data, such as from manual or online tracking tools, mobile apps, and/or data-collecting technology that can be worn, can facilitate not only the partnership, but also better outcomes.
- Formally evaluating the alignment between patients’ and families’ expected outcomes and shared decision making that occurs within TBC partnerships.
- Providing communication training and assessing the impact of effective team communication on patient outcomes.
B. Research opportunities:
- Examining the relationship between effective communication techniques and outcomes data.
- Developing “Navigator” and/or “Team Point Person” programs to assess their impact on improved communication and outcomes.
- Training providers in “motivational interviewing” or strategies to “invite” patients and families into teams and assessing results.
- Assessing patient outcomes in relation to the degree to which they experience partnership with their health care teams.
- Assembling and assessing best practices for ensuring continuity in care and seamless hand-overs between internal and external health care teams that support a “one patient, one team” experience in which the core nucleus of the patient’s team remains intact throughout his/her care experience.
- Developing patient- and family-centered outcome measures that link to effective team-based partnerships and evaluating their use as performance measures.
- Studying the satisfaction of patients, families, and health professionals with outcomes of shared decision-making processes within practices that demonstrate effective partnerships in TBC.
Target: Train leaders for effective team partnerships of patients and health care teams
A. Practice improvements:
- Identifying the characteristics of leaders in organizations that demonstrate effective partnerships of patients and health care teams.
- Establishing accountability at all levels within the practice for patients’ and families’ satisfaction and experience scores.
- Creating rewards for health care teams that have developed excellent partnerships with the majority of their patients who elect to become partners.
- Developing and offering courses for all employees in patient engagement and effective team-based partnerships.
- Basing hiring, evaluation, and promotion on evidence of effective partnership with patients.
- Encouraging the use of electronic medical records and other health information technologies, such as patient portals and shared clinician notes, that promote patient and family health literacy, engagement, and enhanced patient participation as a member of the team.
- Designing spaces that promote partnering with patients as facilities are built and renovated.
- Creating data systems that track patients’ engagement metrics and display graphics in strategic locations for all health care team partners to see and discuss during team meetings.
Accreditation organizations can pursue this goal by:
- Promoting health professions education and continuing education that supports team efforts that include partnerships with patients and families.
- Developing accreditation standards and professional practice guidelines related to fostering TBC and partnerships with patients.
Research opportunities:
- Testing training methods and tools for health care team members to help each one succeed as health care partners.
- Conducting simulation studies involving health professional students at various levels with real or simulated patients to provide a mechanism for collecting early patient satisfaction data and linking them with diagnostic/care accuracy.
- Evaluating the differences among how patients, families, providers, and health system leaders perceive the essential elements of TBC and effective partnerships.
- Collecting information about the views of patients, families, providers, and health system leaders regarding what organizational leadership can do to foster and support effective TBC.
- Developing or using existing continuing education curricula and training focused on teams to support the learning needs of key stakeholders in health care partnerships.
- Testing novel teaching models and including patients as teachers.
- Testing ways of using electronic medical records and other health information technology to facilitate the health team’s effort, including patient portals and shared clinician notes that promote patient and family health literacy and enhanced patient participation in the work of the team.
Appendix B
Summary of the Literature Review
We searched PubMed, Sociological Abstracts, and PsycInfo for journal articles published from 2005 to 2013 that relate primarily to health care teams providing patient-centered care for chronic conditions across the lifespan. The search terms are indicated in the footnote. (PubMed Search Strategies: (patient-centered care[mesh] OR “medical home”[tiab] OR “medical homes”[tiab] OR “patient centerdness”[tiab] OR “patient centeredness”[tiab] OR “patient centered”[tiab] OR patient-centered[tiab]) AND (patient care team[mesh] OR “patient team”[tiab] OR “patient care team”[tiab] OR “health team”[tiab] OR “health care team”[tiab] OR “healthcare team”[tiab] OR “medical team”[tiab]) AND (Patients[mesh] OR Family[Mesh:NoExp] OR Adult Children[Mesh] OR Parents[Mesh] OR Siblings[Mesh] OR Spouses[Mesh] OR Caregivers[Mesh] OR patient[tiab] OR patients[tiab] OR caregiver*[tiab] OR family[tiab] OR families[tiab]) AND (decision making[mesh] OR “decision making”[tiab] OR involvement[tiab] OR participation[tiab] OR role[tiab] OR activation[tiab] OR engagement[tiab] OR member[tiab] OR membership[tiab]) AND (“Health Literacy”[Mesh] OR “Culture”[Mesh:NoExp] OR “Cultural Characteristics”[Mesh] OR “Socioeconomic Factors”[Mesh] OR prejudice[mesh] OR “Language”[Mesh] OR “Health Care Costs”[Mesh] OR “Fear”[Mesh] OR “Anxiety”[Mesh] OR shyness[mesh] OR barrier*[tiab] OR difficult*[tiab] OR literacy[tiab] OR language[tiab] OR fear[tiab] OR anxiety[tiab] OR confusion[tiab] OR education*[tiab] OR culture[tiab] OR cultural[tiab] OR bias[tiab] OR biases[tiab] OR prejudice*[tiab] OR shyness[tiab] OR sterotyp*[tiab])
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Sociological Abstract Search Strategy: ((SU(teamwork OR teams) OR AB,TI(team* OR teamwork)) AND ((AB,TI(“medical home” OR “medical homes” OR “patient centeredness” OR “patient centeredness” OR “patient centered” OR “patient-centered”)) AND SU.explode(literacy OR costs OR culture OR socioeconomic factors OR Rural Communities OR bias OR fear OR anxiety OR ethnicity) OR AB,TI(literacy OR barrier* OR difficult* OR language OR fear* OR anxiety OR confusion OR culture* OR cultural OR bias OR biases OR prejudice* OR shyness OR stereotype* OR education*)
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
PsycInfo Search Strategy: (it=teams OR it=work teams OR ab=team* OR ti=team* OR kw=team*) AND (“medical home*” OR “patient center*” OR patient-center*) AND (patient* OR caregiver* OR famil* OR parent* OR spouse* OR children OR sibling*) AND (decision* OR role* OR engagement OR activation OR member* OR membership OR participation OR involvement) AND (socioeconomic* OR literacy OR barrier* OR difficult* OR language OR fear* OR anxiety OR confusion OR culture* OR cultural OR bias OR biases OR prejudice* OR shyness OR stereotype* OR education* OR costs OR rural)). We reviewed more than 400 abstracts. For journal article abstracts that provided insufficient detail, we reviewed full text. We excluded policy statements, descriptive interprofessional educational curricula on patient-centered care, cost-effectiveness studies, missing abstracts, quality-of-life and feasibility studies, interviews/ surveys/questionnaires of patient perceptions that did not articulate patient roles, and conference grant abstracts and studies in which the role of the patient was not explicitly stated. Thirty-nine studies focused primarily on patient preferences. Sixty-five abstracts were reviewed that described the role of patients and family members on the health care team. We explored the literature on patient-centered care across the lifespan delivered by health care teams that manage chronic or life-limiting illnesses to develop a model for assessment of patient engagement/participation on the health care team. We have organized our summary of the literature in terms of seven questions:
- Are there existing typologies of the various kinds of health care teams and/or of the types of tasks health care teams are established to accomplish? If so, could these different types of teams, or tasks, be stratified around the desired types of patient involvement? (Lead: Veronica Chollette);
- What is the basic knowledge about what makes teams work? Does that need to be adapted for health care settings, and to the roles of patients on teams? (Lead: Richard Ricciardi);
- What are potential roles for patients as members of a health care team? Can these be stratified in a rational way? (Lead: Veronica Chollette);
- What philosophical or ethical bases exist for seeking to integrate patients as team members? What are some assumptions that might underlie these normative arguments? (Lead: Matthew K. Wynia);
- Are there studies on the impact of integrating patients as team members and/or what can be extrapolated from studies on patient activation and engagement? What outcomes have been measured? (Lead: Melissa A. Simon);
- How can the team partner with the patient more effectively to improve patient outcomes? How can the patient’s perspective guide effective treatment goals and activities of team-based care? (Lead: Dale C. Strasser); and
- What are the key facilitators and barriers to integrating patients as team members and, of these, which might be amenable to policy, financing, or structural interventions? (Lead: Pamela H. Mitchell).
Typologies and Kinds of Health Care Team
Veronica Chollette, National Cancer Institute (The views expressed are solely the opinions of the individual and do not necessarily reflect the official policies of the National Cancer Institute, nor does mention of the department or agency names imply endorsement by the federal government.)
Health care clinicians have been encouraged to deliver team-based care and, in the 21st century, such teams have become integral to delivering more effective, more efficient patient care, as was envisioned by the Institute of Medicine (IOM) in its report, Crossing the Quality Chasm. But “evidence-based, patient-centered, and systems-oriented [team-based care] also implies new roles and responsibilities for patients and their families, who must become more aware, more participative, and more demanding in a care system that should be meeting their needs” (IOM, 2001, p. 20).
Our aim is to identify typologies of health care teams and the tasks they are established to accomplish. We also want to determine if the tasks can be stratified around the desired types of patient involvement. For the purpose of this discussion paper, an effective health care partnership includes health providers working in concert with patients and family caregivers to achieve positive experiences and mutually agreed-upon outcomes.
We recognize variability exists among types and tasks of health care teams. Patients may be involved in multiple health care teams and their involvement may not be necessary for all. For example, the tasks of administrative or trauma teams may not require patient involvement.
Team definition and types
As described in Taplin’s May/June 2013 Annals of Family Medicine commentary, “Teams typically are embedded in a larger social system and involve two or more people who differentiate their roles, share common goals, interact with each other, and perform tasks affecting others (Cohen and Bailey, 1997; Lemieux-Charles and McGuire, 2006; Fried, 2012). Within this definition:
- Work teams accomplish tasks on an ongoing basis in a specific organizational setting (e.g., a primary care team, surgical team, emergency department team);
- Parallel teams address shared challenges, such as responding to a cardiac arrest or aiding the transition of patients from hospital care to ambulatory care, and typically draw participants from several work teams;
- Project teams focus on a one-time deliverable and have limited terms (e.g., an electronic health record implementation team); and
- Management teams oversee all the others (Cohen and Bailey, 1997; Lemieux-Charles and McGuire, 2006; Mathieu et al., 2008). Some also argue that within work teams, there are subcategories whose variation in specialty and disciplinary mix may account for much of their success. Differences among teams are important because the tasks that teams undertake, the settings in which they work, and the expectations they face influence their effectiveness” (Lemieux-Charles and McGuire, 2006; Mathieu et al., 2008).
Multiple team types, practices, and patient-centered medical homes (PCMHs) emphasize the significance of patient-centered care in realizing better health outcomes. The specific roles of patients and families as active members of the health care team and evidence of collaboration, however, are scarcely described in manuscript abstracts. Review of full-text articles is necessary to evaluate patient and family roles on the team and measurement of effectiveness if abstract descriptions are vague. Descriptions of patients and families exerting influence in their health could not be exclusively categorized in a taxonomy of any type of health care team (e.g., patient population, disease types, care delivery settings, professional identity, or extreme action teams). For example, patient and family participation in shared decision making (SDM) was observed across intensive care units; Home Health, and Multidisciplinary Care Teams; and various types of physician practices and patient-centered care teams. Vague descriptions of patient and family roles also were noted in manuscript abstracts (see Table B-1, pp. 44-46).
These non-specific roles are characterized as improvement partners, patient involvement, self-reported engagement, effective partnership, and co-managers. Patient and family participation on the team as co-decision makers and the ability to participate in self-management behaviors that improve clinical outcomes appeared frequently, but not exclusively, in Diabetes Care Teams, in PCMHs, in the hospital, and in community settings. Online health communication tools are emerging as acceptable means for information exchange between patients and providers, SDM for co-determined treatments, interventions, and self-management. Health care team tasks are mostly characterized by the delivery of patient-centered care. There is a need to understand task effectiveness (interdependence, outcome interdependence, and team potency) of teams with patients and families as active members and their impact on team functioning. Evaluation of clinical outcomes when patients and family members are on the team is needed. Family members are welcomed and accepted members of the health care team along all points of the health care continuum. Regardless of the type of health care team, patient engagement can enhance team processes and improve clinical outcomes.
Basic Knowledge Regarding Team Work and Role of Patients
Richard Ricciardi, Agency for Healthcare Research and Quality (The views expressed are solely the opinions of the individual and do not necessarily reflect the official policies of the Agency for Healthcare Research and Quality, nor does mention of the department or agency names imply endorsement by the U.S. government.)
Four definitions of teams that are critical to identifying what makes teams work and the role of patients are provided below.
“A team is a collection of individuals who are interdependent in their tasks, who share responsibility for outcomes, who see themselves and who are seen by others as an intact social entity embedded in one or more larger social systems (e.g., business unit or the corporation) and who manage their relationships across organizational boundaries” (Cohen and Bailey, 1997, p. 241).
“A team can be defined as a social system of three or more people, which is embedded in an organization (context) whose members perceive themselves as such and are perceived by members and others (identity), and who collaborate on a common task (teamwork)” (Hoegl and Gemuenden, 2001, p. 436).
“Health care organizations (HCOs) have diverse agents that learn, including providers, patients, and other stakeholders. Diversity is often a source of creativity and problem-solving ability, but can also be a source of communication difficulties. Learning is not one-dimensional, focusing on uncertainty reduction, but it also incorporates learning aimed at uncertainty absorption. Relationships among agents are usually non-linear. Outputs may be disproportional to inputs; small inputs can produce large outcomes; and large inputs can produce small outcomes. Learning by diverse agents, coupled with nonlinear interactions, leads to self-organization, emergence, and co-evolution. Self-organization is the development of dynamic but stable patterns of organization that arise through the local interactions of agents, and in HCOs may include the way that work is allocated or the way equipment use is scheduled. Emergent properties are properties that exist at one level of the organization that cannot be explained by understanding properties at other levels of the organization. Examples of emergent properties in HCOs include patterns of communication between patients and clinicians and levels of trust among medical specialists. Complex Adaptive Systems co-evolve with their environments. Co-evolution occurs when an organization’s response to its environments alters both the organization and the environments, often causing the original response to no longer be adaptive. For example, when a primary care clinic in a community affiliates with a hospital system to capture patients, other clinics in the community often follow suit, and the hospital system may then develop restrictive policies in an attempt to control all of the clinics” (McDaniel et al., 2009, pp. 3-4).



“Team-based health care is the provision of health services to individuals, families, and/or their communities by at least two health providers who work collaboratively with patients and their caregivers—to the extent preferred by each patient—to accomplish shared goals within and across settings to achieve coordinated, high-quality care” (Mitchell et al., 2012, p. 5).
In 2013, a comprehensive review on the evolution of teams and team-based health care was conducted by the Agency for Healthcare Research and Quality (AHRQ), and findings suggest that high-functioning health care teams are characterized by the strength of relationships, processes, and interactions with individuals that form a team (Shoemaker et al., 2013, unpublished). Health care teams include a mix of people and talents and capabilities that perform interdependent functions that fulfill the needs of patients they serve and with whom they partner. The team may be as small as one health care clinician and one patient, but also may include others supporting that patient’s care, including people who aren’t part of the organization or institution. Patients hold a unique and central membership position on the team. All members, including patients, must be aware they are part of a team and participate as part of the team. The necessary conditions that promote team members’ engagement (including patients) and high team functioning include respectful interaction, rich communication, mindfulness, trust, and shared goals. Participatory leadership is a central component and catalyst across all domains of high-functioning health care teams.
In summary, health care teams must communicate in ways to create trust and a mental model that is shared by patients and all team members. Team primacy moves from a state of “me” to “we” with mutually agreed-upon common goals and a high degree of role clarity, including the patient’s role, while successfully confronting any task ambiguities. Future high-functioning health care teams will adapt to meet the patients’ needs and engage the patient in the sequencing of mutually agreed-upon tasks and objectives, ensure a full awareness of who is on the team and what their roles and responsibilities are, allow sufficient time and support for the team to develop, and continuously evaluate and revise patient-centered shared goals.
Roles for Patients as Members of Health Care Team
Veronica Chollette, National Cancer Institute
Health care clinicians have been encouraged to deliver team-based care and, in the 21st century, such teams have become integral to delivering more effective, more efficient patient care, as was envisioned by the IOM in its 2001 report, Crossing the Quality Chasm.
We recognize variability exists among types and tasks of health care teams. Patients may be involved in multiple health care teams and their involvement may not be necessary for all.
Examples of patient roles on the health care team in the review of 65 papers include:
- Participation in group education programs;
- Expressing values and preferences for end-of-life care in team meetings;
- Self-management;
- Knowledge sharing;
- Goal setting;
- Collaboration with the health care team as improvement partners;
- Participation in bedside reporting during shift changes;
- Planning and evaluation of services;
- Participation in care planning process;
- Understanding and using tools to self-monitor health (e.g., pedometer, glucose monitoring, blood pressure); and
- Endorsement of treatment goals.
Participation in shared decision making was cited most frequently as the recurring role of patients and families on the team. This role was noted most in primary care settings; hospitals, clinics, hospice, and community practices; and among patient-centered health care teams.
Patient and family caregiver roles can be stratified according to patient activation, engagement, and membership on the team. Patients and families can be acknowledged as members of the team. Depending on their role or task on the health care team, they may or may not include knowledge of self-care or engagement. For example, a few abstracts describe the need for patient collaboration (welcomed membership) in planning and evaluation of services in continuous quality improvement efforts and implementation to improve factors that enhance collaboration, but knowledge of self-care (activation) or being active in improving one’s health (engagement) is not discussed. Examples of patients and families on the team who are activated and engaged and who have improved clinical outcomes appear frequently in the care of patients with diabetes (see Table B-2, pp. 49-53).




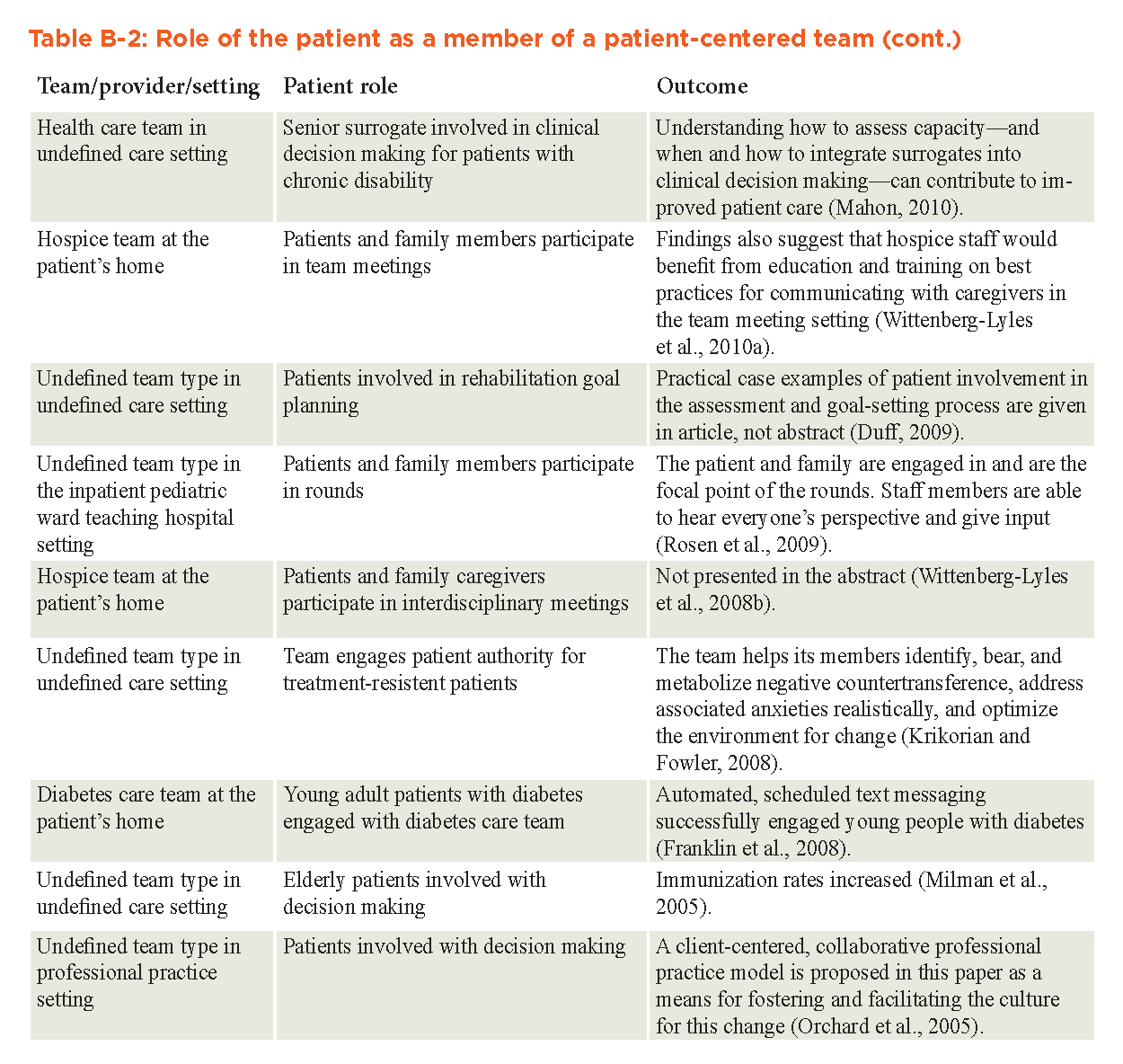
Ethical Considerations for Integrating Patients as Team Members
Matthew W. Wynia, American Medical Association
Ethics are the shared values and standards that guide behavior within and between groups. They are often made explicit in written codes of ethics, but not always. Within health care teams, the ethics of teamwork are commonly implicit, though some health professional codes of ethics address ethical issues in team-based care (Virtual Mentor, 2013; Doherty and Crowley, 2013; AMA, 2014).
In addition, there are some common ethical values that tend to govern the work of high-functioning health care teams. In a prior IOM discussion paper, five values were noted to be shared by members of high-functioning, patient-centered teams (Mitchell et al., 2012) (Table B-3.)
Several papers have explored ethical issues in team-based care, but none explicitly address the ethics of including patients as members of health care teams (Van Norman, 1998; Cassel et al., 2002). Still, a few general observations about the ethics of working in health care teams can be extrapolated to help explore the ethical implications of considering patients to be team members. First, team-based care is rooted in an ethical belief in the importance of shared responsibilities and accountability. (There is no single “captain of the ship” in team-based health care, a fact that has been recognized by a number of courts.) Interdependence, a core concept in team-based care, implies that there are critical performance expectations for every single member of the team. While not overtly considering the roles of patients, ethicists have explored the implications of this basic tenet of teamwork with regard to team members with varying skills and training. As Gail Van Norman, M.D., has written, “Relationships between professionals on the multidisciplinary team are by their nature unequal ones. Different knowledge and experience in specific issues both ethically and legally impart unequal responsibility and authority to those care providers with the most knowledge and experience to handle them. But also because of differences in training and experience, each member of the team brings different strengths” (Van Norman, 1998).
Certainly, having a patient as a team member brings a critical vantage point and unique strengths to help the team accomplish its goals. But it is not clear that all patients can be seen as interdependent team members with accountabilities that are on par with other team members. The most apparent examples are instances during which patients are incapable of decision making or are hindered in their capacity to participate in self-care. Even short of this, some patients will not desire to have other team members hold them accountable for meeting explicit responsibilities, and it is not always clear whether this is reasonable.
Second, teams depend on open communication and honesty among team members. Yet, patients have important privacy rights and might not want to share feelings and experiences with all other team members openly and honestly. In addition, power imbalances can make patients less willing to raise questions or criticize other team members.

Third, high-functioning teams have shared values and goals, yet patients do not always share all of the same goals as other team members, or they might hold different values or interpret goals very differently from other team members. Conflicting goals can relate to religious, cultural, or other belief system differences, or they might simply reflect conflicting priorities. For instance, teams often seek to provide care that is efficient and cost-effective, but research suggests that few patients place high value on wise stewardship of health care resources in the context of their own care (Sommers et al., 2013).
Finally, if there is frequent conflict with one team member, this can lead to a decision to fire the member who doesn’t work well with the rest of the team. For a number of important ethical reasons, there should be a much higher bar for “firing” a patient from a health care team.
Impact of Integrating Patients as Team Members
Melissa A. Simon, Northwestern University
The public health relevance of patient activation is expanding as large numbers of patients are entering a health care system with continued limited resources. Efforts to improve both health care delivery and cost effectiveness in the United States increasingly have begun to focus on addressing particular barriers to care for patients, as well as ways to improve their self-management. Patient activation has emerged as one way to describe, and hopefully to improve, an intangible sense of patient control and self-management. The Patient Activation Measure (PAM) was initially described by Hibbard and colleagues in 2004 as a way to quantify patient activation; their 13-question short form, published in 2005, is now being used by investigators both as a primary outcome and as a predictor for various health interventions (Greenfield et al., 1985; Greenfield et al., 1988). Activation has been shown to be correlated with both health behaviors and health outcomes. A 2012 study by Greene and Hibbard found that for every additional 10 points on the PAM scale, the probability of smoking, being obese, or having an emergency department visit was 1 percent lower, whereas the likelihood of having normal hemoglobin A1c, high-density lipoprotein, or triglycerides, or of having had a mammogram, was 1 percent higher.
Activation is particularly relevant for public health interventions because it has been shown to be lower in many groups with lower health outcomes, who are traditionally more difficult to connect to health care resources. Thus, it represents potential opportunities to identify individuals who may struggle with self-management of their health and to explore which types of interventions may help them improve self-management in the future, especially in a system that increasingly will demand it.
Previously, PAM scores have been shown to be lower in Latinos and African Americans, as compared with whites; adjusting for demographic variables and socioeconomic status erased much of the difference between African Americans and whites, but not between Latinos and non-Hispanic whites, indicating that differences may have been more affected by immigration and language factors (Kaplan et al., 1995). In a patient activation study focused exclusively on Latinos, activation was found to be higher in U.S.-born and bilingual Latinos than in foreign-born or exclusively Spanish-speaking patients (Jahng et al., 2005). Lubetkin et al., in 2010 found that better-educated patients were more activated, as were patients with adequate health literacy and better self-rated health, as we might expect from the PAM questions (Haskard et al., 2008). Additionally, Mosen et al. found that not only were their study patients with higher PAM scores more likely to perform self-management behaviors and report medication compliance, but they also were more likely to report high patient satisfaction, quality of life, and physical and mental functioning scores (Street et al., 2005). Finally, activation previously has been shown to be correlated with better quality of care and communication with physicians, even after controlling for demographics and language (Jahng et al., 2005). A number of studies have demonstrated the ability to increase PAM through a variety of interventions (coaching/counseling, online wellness portals, obesity programs, workshops, etc.) (Kaplan et al., 1989; Cegala, 2003; Cegala et al., 2007; Cegala and Post, 2009; Cegala et al., 2012, 2013). One study found that in older adults with chronic disease (diabetes or heart disease), 52 percent of patients’ activation levels changed at one-year follow-up (without an intervention); 54 percent increased and 46 percent decreased (Post et al., 2002).
Of particular importance is whether the increase in activation then corresponds to increasing performance of certain health behaviors. A small number of studies already have begun to explore this issue; many of them have been able to improve PAM scores, although at times the scores of control groups improved as well, and the related increase in health behaviors has not been expanded yet to demonstrating improved health outcomes. Shively and colleagues designed an intervention in which advanced practice nurses developed individualized plans for coaching/counseling patients diagnosed with heart failure based on their baseline activation stage (Shively et al., 2013). They significantly increased PAM scores over the six-month intervention period (especially for patients with medium levels of baseline activation), as well as adherence to health behaviors, but were not able to show a consistent decrease in hospitalizations for these individuals (Smith et al., 2013). Hibbard and colleagues published an article examining the Chronic Disease Self-Management Program (weekly workshops for six weeks), which attempted to increase patient activation and to study whether that increase in activation was associated with improved health behavior performance. Activation increased in both the intervention and the control group (although more quickly in the intervention group); they could not draw strong conclusions about effective ways to improve activation. However, they did demonstrate that with improved activation, there was improved performance of a number of baseline health behaviors (including exercising, managing stress, monitoring dietary fat, monitoring home blood pressure and glucose, and taking recommended diabetes medications), even among some participants who weren’t performing such activities at the beginning of the study (Cegala, 2003; Hibbard et al., 2007; Hibbard et al., 2009). A similar study compared an activated consumer program (seminars and coaching on evaluating health information, preventive guidelines, and importance of taking medications as prescribed) to a traditional health promotion program and to a control group. They found that PAM increased significantly, with a mean change of 4.31. Those at level 1 at baseline improved the most (average increase of 17). Overall, these increases were related to a decreased health risk score for patients, and specifically to improved aerobic exercise, safety, and frequency of breakfast, and to decreased stress and lowered cancer risk (Epstein and Street, 2011).
In summary:
- Patient-centeredness and integrating patients on the team leads to better outcomes. Team functioning predicts patient outcomes.
- TeamSTEPPS and other models have been useful in health education (AHRQ, 2014b).
- The power of the electronic health record has been addressed somewhat in terms of making computer templates that would detail the process of the team and the involvement of patients.
- There is wide variation within teams, and a certain chemistry is required for teams to work. Several barriers can impact the team dynamics—including personalities and the environment. There can be a naiveté about integrating the patient into the team; one cannot think about it in the same way as incorporating a more technical part of the staff into the team. However, patients bring technical skills in their own right.
- Studies outside the field of medicine show that diverse groups are more innovative and creative than monolithic groups.
Team Partnering with Patients to Improve Outcomes
Dale C. Strasser, Emory University Medical School
Extensive literature exists to support the superiority of team-based care and increased care coordination across a spectrum of settings and medical specializations. Team-based care emerged concurrent with the development of geriatrics, rehabilitation medicine, public health, and mental health (Rusk, 1972; Mathews, 1984). In stroke rehabilitation, for example, the value of team-based care and dedicated stroke units have been endorsed widely, are written into accreditation standards, and are referenced by regulatory agencies (Duncan et al., 2005; CARF, 2013). Furthermore, reviews on the topic across settings support team care while simultaneously acknowledging the challenges of realizing its potential. Team-based care plays a major role in the IOM work on quality and patient safety, including the landmark report, Crossing the Quality Chasm (IOM, 2001).
The background and justification for team-based health care is summarized in the Core Principles and Values of Effective Team-Based Health Care discussion paper (Mitchell et al., 2012). For the early adopters of team-based care (e.g., geriatrics and rehabilitation), the impetus for an interdisciplinary approach arose in contrast to the existing medical model as a way to address patient-centered goals more directly. Although the assumption that team-based care promotes (or has the potential to promote) greater patient-centered care is reasonable, it merits further study and refinement.
This section examines “how” team care impacts outcomes. The relationship of Team Functioning (TF) to patient outcomes resides at the core.
TF refers to the “skill and reliability with which team members work together” (Mitchell et al., 2012, p. 3). The spectrum of TF runs from “parallel practice, in which clinicians mostly work separately, to integrative care, in which the interdisciplinary team approach is pervasive and non-hierarchical and utilizes consensus building, with variations along the way.” Common sociobehavioral themes (e.g., communication, discipline boundaries, leadership, and goal-directed) run through the diverse literature on teams. Hence, the partnership between the team and the patient can be operationalized as the sociobehavioral characteristics of teams that impact patient outcomes.
Potentially modifiable variables
This section discusses potentially modifiable variables of TF extrapolated from existing research, and is organized along the lines of the conceptual model of treatment effectiveness in stroke rehabilitation developed in 1997 by Strasser and Falconer (Smits et al., 2014). This model provided the conceptual framework for the Department of Veterans Affairs (VA) Rehab Teams Project (VA Merit E1101R; B2367R; O3225R), a 15-year effort examining team functioning and patient outcomes. This model was developed to guide clinician-centered research linking TF to patient outcomes.
The model posits that team care mediates between system inputs (hospital organization, treatment/technologies, and participants) and patient outcomes. TF is based on team actions and team relations. Team actions are conceptualized along a spectrum anchored by team leadership at one extreme and managerial practices at the other. Likewise, team relations are seen as a spectrum anchored by social climate (e.g., interprofessional relations on a team) and professional networks (e.g., interprofessional relations of team function).
Modifiable variables: Which interventions work?
In a cluster randomized trial of team training for stroke rehabilitation, Strasser et al. (2008) tested whether a team training intervention in process improvement would be associated with improved outcomes for stroke patients over a one-year period. The team training consisted of a six-month staff education intervention centered on a 2.5-day workshop for two self-identified team leaders from each intervention site. Prior to the intervention, both groups received a customized TF portrait. This portrait compared the participant’s specific team characteristics to national norms and offered interruptive comments on the findings. The primary outcome was improvement in function. Stroke patients treated by the experimental group had statistically greater gains than patients in the control group. These findings support the use of staff education and skills development that target relevant clinical issues, along with peer feedback on self-identified barriers, site-specific action plans, and an empirical model consistent with clinical experience (Stevens et al., 2007).
To summarize, the general thesis that TF impacts outcomes is well supported. More specifically, a growing body of literature finds that TF can be characterized in socio-behavioral constructs and that different attributes of TF (e.g., managerial practices, professional networks) are associated with different outcomes (e.g., functional gain, community discharge). Of interest, the specific impact of TF interventions relates to the particular TF attribute addressed. Strasser and colleague’s (2008) clinical trial supports the value of direct clinician engagement on relevant aspects of TF associated with a self-identified problem.
The nature of team care
By its nature, team care is both subtle and complex. The chemistry underlying effective teams varies by tasks, settings, and personnel. In one instance, a pivotal issue may be smooth interprofessional relations while, in another instance, social climate or physician engagement may be critical. In Alexander and colleague’s longitudinal study of 40 VA mental health teams (2005), effective team functioning involved active patient engagement and not necessarily smooth-running teams. One can imagine a smooth-running team disengaged from the patient (e.g., not patient-centered care), which has limited, even detrimental, impact on outcomes. These findings suggest a dynamic interplay between team care and patient engagement.
The challenges of methodology and measurement in researching this area reflect the complexity of the topic. For example, the high intercorrelations of both TF measures and outcomes (patient, team process, organizational-financial) mean that specific relations must be interpreted cautiously. This complexity may partially explain the limited direct research on TF and patient-centered care. Patient engagement, including team-based care, presupposes clear communication and implementation approaches. A high-functioning team commonly arrives at that stage of engagement after internally processing the patient’s circumstances. There are usually some starts and stops along the way.
A patient cannot be a member of the team in the exact same manner as a trained health professional. As well, by definition, patients requiring team care are vulnerable because they are sick or have a chronic condition. This may differ for patients with stable conditions requiring simpler clinical decision making, like that which can be made in a straightforward outpatient visit with a primary care physician. Rather than integrating patients as team members, more useful framing questions could be:
- How can the patient’s perspective guide effective treatment goals and activities of team-based care? and
- What aspects of TF impact patient-centered care and how can they be improved?
Basic principles of group and team process provide insights into this team partnership with the patient. Diversity in groups promotes broader, more innovative results. It is generally recognized that more diverse work groups, such as by age, gender, ethnicity, and professional background, result in more creative and generally effective solutions than groups dominated by one gender or ethnicity. It is likely that a similar dynamic occurs on interdisciplinary patient care teams. The diversity of professional backgrounds along with usual diversity in age, gender, and ethnicity provides more opportunities for meaningful engagement between clinicians and patients. Shared leadership tasks may default to the clinician who connects best with a given patient in a particular circumstance. Effective teams flow with this dynamic for optimal results.
Key Facilitators and Barriers to Integrating Patients on Teams
Pamela H. Mitchell, University of Washington
The AHRQ search produced 231 citations using keywords and databases cited in the evidence base that appears on p. 40. This section summarizes the 28 citations in our review that were based on some type of systematic inquiry and included patient/family perspective. Most commonly, these were single or multiple case reports using mixed methods (interviews, surveys, observation) of primary care practices. However, psychiatric and rehabilitation teams were reported on the second most frequently. There was one cluster randomized trial of collaborative care that explicitly included patients/families with their clinician team (Dobscha et al., 2009). Although this trial demonstrated significantly improved patient outcomes from chronic pain management, facilitators and barriers to collaborative care processes were not reported. One group had several reports on different palliative care and hospice teams that explicitly included analysis of patient-family-team interactions (Wittenberg-Lyles, 2005; Wittenberg-Lyles et al., 2008a; Wittenberg-Lyles et al., 2008b; Wittenberg-Lyles et al., 2010a; Wittenberg-Lyles et al., 2010b; Wittenberg Lyles et al., 2012). Fennel and colleague’s review of organizational influences on quality team care and Greenhalgh and colleague’s concept analysis indirectly help illuminate facilitators or barriers (Fennel et al., 2010; Greenhalgh et al., 2009).
The majority of the papers reported facilitators to integrating patients on teams (see Table B-4, pp. 62-65):
- Team-based care;
- Improved communication within the team;
- Feedback to clinicians;
- Family-centered care with parents as improvement partners;
- Cultural awareness;
- Keeping families together;
- Treating patients with respect;
- Showing care and concern; and
- Patient-centered care with explicit patient involvement, active listening, and a culture of quality improvement and shared learning (Bunniss and Kelly, 2008; Davies et al., 2008; Mercer et al., 2008; Chan et al., 2010; Brierley et al., 2012; Carr et al., 2012; Foster et al., 2012; Markova et al., 2012; Wittenberg-Lyles et al., 2012; McAllister et al., 2013).




When barriers to integrating patients on teams were mentioned, they usually were implied as lack of the facilitators (see Table B-4, pp. 62-65). However, explicit barriers noted included:
- Poor team cohesion;
- Differences in consultative style;
- Poor communication, including lack of training in communication;
- Emphasis on medical model (versus biopsychosocial model);
- Patient perception of being disrespected;
- Mechanical behavior of staff;
- Lack of leadership commitment (from larger organization or practice);
- Isolation of physicians from rest of staff;
- Isolation of decision-makers in acute settings;
- Information overload; and
- Lack of time for team briefings, improvement, and professional support (Chesluk and Holmboe, 2010; Miller et al., 2010; Wittenberg-Lyles et al., 2010a; Brierley et al., 2012; Carr et al., 2012; Markova et al., 2012; Wittenberg-Lyles et al., 2012; Körner et al., 2013; McAllister et al., 2013; Watt et al., 2013).
Additional barriers included poor conflict management, physical layout precluding team communication, not involving the patient as much as he or she wants, lack of experience in using feedback and data, and absent or inadequate staffing for care coordination (Davies et al., 2008; Mercer et al., 2008; Oandasan et al., 2009; Körner et al., 2013; McAllister et al., 2013).
Appendix C
Jessie Gruman, Sandra Leal, Beth A. Lown, Carly Parry, and Ron Stock
Interview Guide
Introduction
Can you please confirm that you have agreed to have this interview recorded?
Hello and welcome. We are here today to discuss your opinions about and experiences with team-based health care.
My name is […]. I represent the Best Practices Innovation Collaborative, volunteer participants working to improve patient care.
I am taking notes. In addition to taking notes, we are recording this session because we want to make sure that we capture everything that you would like to tell us. All of your responses will be confidential and any mention of personally identifying information, such as your name, will not be included in the transcript. After the written transcript is verified for accuracy, the recording will be promptly destroyed. You can also ask us to stop at any time if you no longer want to participate. Your decision to participate will not affect your care.
The interview will take about 25 to 30 minutes.
It’s important to remember that there is no “right” or “wrong” answer. We’re interested in learning about your experiences.
Increasingly, health care is provided by a team of health care professionals, such as doctors, nurse practitioners, nurses, medical assistants and technicians, and even pharmacists, dieticians, dentists, social workers, case managers, and other staff. In this team-based health care model, a team of health care professionals work together, and with patients, to prevent or treat health conditions.
We want to know about your opinions about and experiences with these types of health care teams. What works? What doesn’t work? And what team members could do differently to improve your care?
Are you ready to begin?
Q1: First of all, where do you currently get most of your health care needs met? Would that be [name of referring institution] or somewhere else?
Probes:
- How often do you visit [name of referring institution]?
- Overall, in the last six months, approximately how many different health care practitioners have you seen, such as doctors, nurses, physical therapists, etc., including people at [name of referring institution] and elsewhere?
Q2: At [insert name of referring institution] do you feel like you (are/were) treated by a team? Do you feel like it (is/was) a team-based approach to your care?
Q3 TO BE ASKED OF THOSE WHO SAID “YES” OR “MOSTLY” TO Q2
Q3: When you think about health care provided by a “team” at [name of referring institution], what indicates to you that you are being treated by a team?
Probes:
- Who are the main members of your health care team, as you see it?
- Are there other health care practitioners or other staff at [name of referring institution] who are involved in your care?
- What are the different health care services and treatments you receive from the different team members? Who does what?
- Has [name of referring institution] provided other services, supports, help, or resources? If so, what?
- How does your health care team coordinate or manage your health care needs?
- Does the team work together to come up with a plan for your care?
- How do the team members communicate with each other and with you?
- Is there a patient portal where you can go to look at your records, get test results, or make appointments? If so, tell me about that.
Q4 TO BE ASKED OF THOSE WHO SAID “YES,” “MOSTLY,” OR “SUPPOSEDLY” TO Q3
Q4: Overall, how good a job does [name of referring institution] do at delivering team care to you as a patient?
Probes:
- How, if at all, did [name of referring institution] do a good job delivering team care? In what ways was it good/successful?
- How, if at all, did they fall short?
ASK Q5 OF ALL
Q5: Do you feel that you are involved in your health care in a way that meets your needs?
Probes:
- IF NO: What would make it better?
- IF YES: What needs are being met now? How is that happening?
- ASK THOSE WHO SAID YES OR MOSTLY TO Q3: To what extent do you feel that you are part of your health care team? If yes, how so?
- ASK THOSE WHO SAY THEY DO CONSIDER THEMSELVES A MEMBER OF THE TEAM: Overall is you being a member of the team a good thing or a bad thing for you as a patient?
- How so?
INTRO TO Q6 FOR THOSE WHO SAY THEY HAVE NOT RECEIVED TEAM CARE IN Q3: In the team-based health care model, health care is provided by a team of health care professionals, including doctors, nurse practitioners, nurses, medical assistants and technicians, and even pharmacists, dieticians, dentists, social workers, case managers, and other staff. The idea is that the team members work together, and with patients, to prevent or treat health conditions. Based on this description…
ASK Q6 OF ALL
Q6: Overall, do you feel team-based health care is good or bad for patients?
Probes:
- What, if anything, is/might be good for patients about team-based care? How does it benefit patients?
- ASK THOSE WHO HAVE RECEIVED TEAM CARE: How has it benefited you? How does it improve your care and your experience as a patient?
- What, if anything, is/might be bad for patients about team-based care? How does/might it harm, or fail to help, patients?
- ASK THOSE WHO HAVE RECEIVED TEAM CARE: How, if at all, has it harmed or failed to help you?
ASK OF THOSE WHO HAVE SAY THEY HAVE NOT RECEIVED TEAM CARE IN Q3:
Q7: What do you think it would mean for you, as a patient, to be considered as an actual “member of your health care team?”
Probes:
- What would your role be? What would your responsibilities be?
- Would you like to be a member of your health care team?
- Why/why not?
- What would be good about being a member of your health care team?
- What would be bad about being a member of your health care team?
Q8: What would you consider the ideal way to provide for your health care needs?
Probes:
- Imagine the ideal experience of getting your health care needs met. What would that look like?
- How would this be different from the care you receive now at [name of referring institution]?
- Would this ideal involve team-based health care?
Q9: Is there anything else about (your experience with or) the idea of health care provided by a team that we haven’t discussed that you’d like us to know about?


References
- AHRQ (Agency for Healthcare Research and Quality). 2014a. Multiple chronic conditions. Available at: http://www.ahrq.gov/professionals/prevention-chronic-care/decision/mcc/index.html (accessed July 7, 2014).
- AHRQ. 2014b. TeamSTEPPS national implementation. Available at: http://www.teamsteppsportal.org/ (accessed October 6, 2014).
- Alexander, J., R. Lichtenstein, K. Jinnett, R. Wells, J. Zazzali, and D. Liu. 2005. Cross-functional team processes and patient functional improvement. Health Services Research 40(5 Pt 1):1335-1355. https://doi.org/10.1111/j.1475-6773.2005.00418.x
- Alston, C., L. Paget, G. Halvorson, B. Novelli, J. Guest, P. McCabe, K. Hoffman, C. Koepke, M. Simon, S. Sutton, S. Okun, P. Wicks, T. Undem, V. Rohrbach, and I. Von Kohorn. 2012. Communicating with Patients on Health Care Evidence. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201209d
- AMA (American Medical Association). 2014. AMA adopts policy to define team-based health care. Available at: http://www.ama-assn.org/ama/pub/news/news/2014/2014-06-09-policy-to-define-team-based-medicalcare.page (accessed October 2, 2014).
- American Academy of Pediatrics’ Committee on Hospital Care and Institute for Patient- and Family-Centered Care. 2012. Patient- and family-centered care and the pediatrician’s role. Pediatrics 129(2):394-404. https://doi.org/10.1542/peds.2011-3084
- Anderson, B. 2007. Collaborative care and motivational interviewing: Improving depression outcomes through patient empowerment interventions. American Journal of Managed Care 13(4 Suppl):S103-S106. Available at: https://pubmed.ncbi.nlm.nih.gov/18041866/
- Anderson, C., and R. Mangino. 2006. Nurse shift report: Who says you can’t talk in front of the patient? Nursing Administration Quarterly 30(2):112-122. https://doi.org/10.1097/00006216-200604000-00008
- Aschner, P., J. LaSalle, and M. McGill. 2007. The team approach to diabetes management: Partnering with patients. International Journal of Clinical Practice Supplement (157):22-30. https://doi.org/10.1111/j.1742-1241.2007.01606.x
- Bailey Jr., D., F. Armstrong, A. Kemper, D. Skinner, and S. Warren. 2009. Supporting family adaptation to presymptomatic and “untreatable” conditions in an era of expanded newborn screening. Journal of Pediatric Psychology 34(6):648-661. https://doi.org/10.1093/jpepsy/jsn032
- Beal, A., M. Doty, S. Hernandez, K. Shea, and K. Davis. 2007. Closing the divide: How medical homes promote equity in health care—Results from the Commonwealth Fund 2006 Health Care Quality Survey. New York: The Commonwealth Fund. Available at: https://www.commonwealthfund.org/publications/fund-reports/2007/jun/closing-divide-how-medical-homes-promote-equity-health-care (accessed June 24, 2020).
- Bodenheimer, T., E. Wagner, and K. Grumbach. 2002. Improving primary care for patients with chronic illness: The chronic care model, part 2. JAMA 288:1909-1914. https://doi.org/10.1001/jama.288.15.1909
- Bomba, P., and D. Vermilyea. 2006. Integrating POLST into palliative care guidelines: A paradigm shift in advance care planning in oncology. Journal of the National Comprehensive Cancer Network 4(8): 819-829. https://doi.org/10.6004/jnccn.2006.0069
- Boulding, W., S. Glickman, M. Manary, K. Schulman, and R. Staelin. 2011. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. American Journal of Managed Care 17(1):41-48. Available at: https://pubmed.ncbi.nlm.nih.gov/21348567/ (accessed June 24, 2020).
- Brierley, S., C. Eiser, B. Johnson, V. Young, and S. Heller. 2012. Working with young adults with Type 1 diabetes: Views of a multidisciplinary care team and implications for service delivery. Diabetic Medicine 29(5):677-681. https://doi.org/10.1111/j.1464-5491.2012.03601.x
- Browning, D., and M. Solomon. 2005. The initiative for pediatric palliative care: An interdisciplinary educational approach for healthcare professionals. Journal of Pediatric Nursing 20(5):326-334. https://doi.org/10.1016/j.pedn.2005.03.004
- Brownson, C., D. Miller, R. Crespo, S. Neuner, J. Thompson, J. Wall, S. Emont, P. Fazzone, E. Fisher, and R. Glasgow. 2007. A quality improvement tool to assess self-management support in primary care. Joint Commission Journal on Quality and Patient Safety 33(7):408-416. https://doi.org/10.1016/s1553-7250(07)33047-x
- Bruner, P., M. Davey, and R. Waite. 2011. Culturally sensitive collaborative care models: Exploration of a community-based health center. Families, Systems, & Health 29(3):155-170. https://doi.org/10.1037/a0025025
- Bunniss, S., and D. Kelly. 2008. ‘The unknown becomes the known’: Collective learning and change in primary care teams. Medical Education 42(12):1185-1194. https://doi.org/10.1111/j.1365-2923.2008.03159.x
- Burton, J., E. Murphy, and P. Riley. 2010. Primary immunodeficiency disease: A model for case management of chronic diseases. Professional Case Management 15(1):5-10, 12-14; quiz 15-16. https://doi.org/10.1097/NCM.0b013e3181b5dec4
- CARF–CCAC. Standards Manual. 2013. Available at: http://www.carf.org/WorkArea/DownloadAsset.aspx?id=23968 (accessed December 17, 2013).
- Carman, K., P. Dardess, M. Maurer, S. Sofaer, K. Adams, C. Bechtel, and J. Sweeney. 2013. Patient and family engagement: A framework for understanding the elements and developing interventions and policies. Health Affairs 32(2):223–231. https://doi.org/10.1377/hlthaff.2012.1133
- Carr, E., L. Worswick, P. Wilcock, C. Campion-Smith, and D. Hettinga. 2012. Improving services for back pain: Putting the patient at the centre of interprofessional education. Quality in Primary Care 20(5):345-353. Available at: https://pubmed.ncbi.nlm.nih.gov/23114002/ (accessed June 24, 2020).
- Cassel, C., M. Mezey, M. Bottrell, K. Hyer, and J. Howe. (Eds.). 2002. An ethics casebook in geriatric interdisciplinary team training. Baltimore, MD: The Johns Hopkins Press.
- CDC (Centers for Disease Control and Prevention). 2009. Chronic diseases: The power to prevent, the call to control. Available at: http://www.cdc.gov/chronicdisease/resources/publications/aag/chronic.htm (accessed April 17, 2014).
- Cegala, D. 2003. Patient communication skills training: A review with implications for cancer patients. Patient Education and Counseling 50(1):91-94. https://doi.org/10.1016/s0738-3991(03)00087-9
- Cegala, D., and D. Post. 2009. The impact of patients’ participation on physicians’ patient-centered communication. Patient Education and Counseling 77(2):202-208. https://doi.org/10.1016/j.pec.2009.03.025
- Cegala, D., R. Street Jr., and C. Clinch. 2007. The impact of patient participation on physicians’ information provision during a primary care medical interview. Healthcare Communications 21(2):177-185. https://doi.org/10.1080/10410230701307824
- Cegala, D., D. Chisolm, and B. Nwomeh. 2012. Further examination of the impact of patient participation on physicians’ communication style. Patient Education and Counseling 89(1):25-30. https://doi.org/10.1016/j.pec.2012.03.022
- Cegala, D., D. Chisolm, and B. Nwomeh. 2013. A communication skills intervention for parents of pediatric surgery patients. Patient Education and Counseling 93(1):34-39. https://doi.org/10.1016/j.pec.2013.03.015
- Chan, B., D. Perkins, Q. Wan, N. Zwar, C. Daniel, P. Crookes, and M. Harris. 2010. Finding common ground? Evaluating an intervention to improve teamwork among primary health-care professionals. International Journal for Quality in Health Care 22(6):519-524. https://doi.org/10.1093/intqhc/mzq057
- Chesluk, B., and E. Holmboe. 2010. How teams work—or don’t—in primary care: A field study on internal medicine practices. Health Affairs 29(5):874-879. https://doi.org/10.1377/hlthaff.2009.1093
- Clarke, D., K. Werestiuk, A. Schoffner, J. Gerard, K. Swan, B. Jackson, B. Steeves, and S. Probizanski. 2012. Achieving the ‘perfect handoff’ in patient transfers: Building teamwork and trust. Journal of Nursing Management 20(5):592-598. https://doi.org/10.1111/j.1365-2834.2012.01400.x
- Cohen, S., and D. Bailey. 1997. What makes teams work: Group effectiveness research from the shop floor to the executive suite. Journal of Management 23:239-289. Avaialble at: https://ceo.usc.edu/1996/12/16/what-makes-teams-work-group-effectiveness-research-from-the-shop-floor-to-the-executive-suite/ (accessed June 24, 2020).
- Collins, L., C. Arenson, C. Jerpbak, P. Kane, R. Dressel, and R. Antony. 2011. Transforming chronic illness care education: A longitudinal interprofessional mentorship curriculum. Journal of Interprofessional Care 25(3):228-230. https://doi.org/10.3109/13561820.2011.552815
- Darwish, A., G. Salmon, A. Ahuja, and L. Steed. 2006. The community intensive therapy team: Development and philosophy of a new service. Clinical Child Psychology and Psychiatry 11(4):591-605. https://doi.org/10.1177/1359104506067880
- Davies, E., D. Shaller, S. Edgman-Levitan, D. Safran, G. Oftedahl, J. Sakowski, and P. Cleary. 2008. Evaluating the use of a modified CAHPS® survey to support improvements in patient-centered care: Lessons from
a quality improvement collaborative. Health Expectations: An International Journal of Public Participation in Health Care & Health Policy 11(2):160-176. https://doi.org/10.1111/j.1369-7625.2007.00483.x - Diedhiou, A., J. Probst, J. Hardin, A. Martin, and S. Xirasagar. 2010. Relationship between presence of a reported medical home and emergency department use among children with asthma. Medical Care Research and Review 67(4):450-475. https://doi.org/10.1177/1077558710367735
- Dijkstra, R., J. Braspenning, Z. Huijsmans, R. Akkermans, E. van Ballegooie, P. ten Have, T. Casparie, and R. Grol. 2005. Introduction of diabetes passports involving both patients and professionals to improve hospital outpatient diabetes care. Diabetes Research and Clinical Practice 68(2):126-134. https://doi.org/10.1016/j.diabres.2004.09.020
- Dobscha, S., K. Corson, N. Perrin, G. Hanson, R. Leibowitz, M. Doak, K. Dickinson, M. Sullivan, and M. Gerrity. 2009. Collaborative care for chronic pain in primary care: A cluster randomized trial. Journal of the American Medical Association 301(12):1242-1252. https://doi.org/10.1001/jama.2009.377
- Doherty, R., and R. Crowley, for the Health and Public Policy Committee of the American College of Physicians. 2013. Principles supporting dynamic clinical care teams: An American College of Physicians position paper. Annals of Internal Medicine 159(9):620-626. https://doi.org/10.7326/0003-4819-159-9-201311050-00710
- Doss, S., P. DePascal, and K. Hadley. 2011. Patient–nurse partnerships. Nephrology Nursing Journal 38(2): 115-124; quiz 125. Available at: https://pubmed.ncbi.nlm.nih.gov/21520690/ (accessed June 24, 2020).
- Duff, J. 2009. Team assessment in stroke rehabilitation. Topics in Stroke Rehabilitation 16(6):411-419. https://doi.org/10.1310/tsr1606-411
- Duncan, P., R. Zorowitz, B. Bates, J. Choi, J. Glasberg, G. Graham, R. Katz, K. Lamberty, and D. Reker. 2005. Management of adult stroke rehabilitation care: A clinical practice guideline. Stroke 36:e100-e143. https://doi.org/10.1161/01.STR.0000180861.54180.FF
- Durston, P. 2006. Partners in caring: A partnership for healing. Nursing Administration Quarterly 30(2): 105-111. https://doi.org/10.1097/00006216-200604000-00007
- Dyer, D. 1984. Team research and team training: A state-of-the-art review. Human Factors Review 285-319. https://doi.org/10.1016/0003-6870(85)90133-4
- Ekwall, E., B. Ternestedt, B. Sorbe, and U. Graneheim. 2011. Patients’ perceptions of communication with the health care team during chemotherapy for the first recurrence of ovarian cancer. European Journal of Oncology Nursing 15(1):53-58. https://doi.org/10.1016/j.ejon.2010.06.001
- Epstein, R., and R. Street Jr. 2011. Shared mind: Communication, decision making, and autonomy in serious illness. Annals of Family Medicine 9(5):454-461. https://doi.org/10.1370/afm.1301
- Erlich, D., D. Slawson, and A. Shaughnessy. 2013. Diabetes update: Population management. FP Essentials 408:25-33. Available at: https://pubmed.ncbi.nlm.nih.gov/23690376/ (accessed June 24, 2020).
- Fagerlin, A., K. Sepucha, M. Couper, C. Levin, E. Singer, and B. Zikmund-Fisher. 2010. Patients’ knowledge about 9 common health conditions: The DECISIONS survey. Medical Decision Making 30:35S-52S. https://doi.org/10.1177/0272989X10378700
- Fennell, M., I. Das, S. Clauser, N. Petrelli, and A. Salner. 2010. The organization of multidisciplinary care teams: Modeling internal and external influences on cancer care quality. Journal of the National Cancer Institute (40):72-80. https://doi.org/10.1093/jncimonographs/lgq010
- Fleissig, A., V. Jenkins, S. Catt, and L. Fallowfield. 2006. Multidisciplinary teams in cancer care: Are they effective in the U.K.? The Lancet Oncology 7(11):935-943. https://doi.org/10.1016/S1470-2045(06)70940-8
- Fletcher, K., S. Furney, and D. Stern. 2007. Patients speak: What’s really important about bedside interactions with physician teams. Teaching and Learning in Medicine 19(2):120-127. https://doi.org/10.1080/10401330701332193
- Foster, A., J. Armstrong, A. Buckley, J. Sherry, T. Young, S. Foliaki, T. James-Hohaia, A. Theadom, and K. McPherson. 2012. Encouraging family engagement in the rehabilitation process: A rehabilitation provider’s development of support strategies for family members of people with traumatic brain injury. Disability and Rehabilitation 34(22):1855-1862. https://doi.org/10.3109/09638288.2012.670028
- Fox, P., P. Porter, S. Lob, J. Holloman Boer, D. Rocha, and J. Adelson. 2007. Improving asthma-related health outcomes among low-income, multiethnic, school-aged children: Results of a demonstration project that combined continuous quality improvement and community health worker strategies. Pediatrics 120(4):e902-e911. https://doi.org/10.1542/peds.2006-1805
- Franklin, V., A. Greene, A. Waller, S. Greene, and C. Pagliari. 2008. Patients’ engagement with “Sweet Talk”—A text messaging support system for young people with diabetes. Journal of Medical Internet Research 10(2):126-135. https://doi.org/10.2196/jmir.962
- Fried, B. 2012. Teams and team effectiveness in health services organizations. Shortell & Kaluzny’s health care management; Organization design & behavior. Clifton Park, NJ: Delmar, Cengage Learning.
- Fromer, L. 2011. Implementing chronic care for COPD: Planned visits, care coordination, and patient empowerment for improved outcomes. International Journal of Chronic Obstructive Pulmonary Disease 6:605-614. https://doi.org/10.2147/COPD.S24692
- Glasgow, R., P. Dickinson, L. Fisher, S. Christiansen, D. Toobert, B. Bender, L. Dickinson, B. Jortberg, and P. Estabrooks. 2011. Use of RE-AIM to develop a multi-media facilitation tool for the patient-centered medical home. Implementation Science 6:118. https://doi.org/10.1186/1748-5908-6-118
- Greene, J., and J. Hibbard. 2011. Why does patient activation matter? An examination of the relationships between patient activation and health-related outcomes. Journal of General Internal Medicine 27(5):520-526. https://doi.org/10.1007/s11606-011-1931-2
- Greenfield, S., S. Kaplan, and J. Ware Jr. 1985. Expanding patient involvement in care. Effects on patient outcomes. Annals of Internal Medicine 102(4):520-528. https://doi.org/10.7326/0003-4819-102-4-520
- Greenfield, S., S. Kaplan, J. Ware Jr., E. Yano, and H. Frank. 1988. Patients’ participation in medical care: Effects on blood sugar control and quality of life in diabetes. Journal of General Internal Medicine 3(5):448-457. https://doi.org/10.1007/BF02595921
- Greenhalgh, T., C. Humphrey, J. Hughes, F. Macfarlane, C. Butler, and R. Pawson. 2009. How do you modernize a health service? A realist evaluation of whole-scale transformation in London. Milbank Quarterly 87(2):391-416. https://doi.org/10.1111/j.1468-0009.2009.00562.x
- Han, E., S. Hudson Scholle, S. Morton, C. Bechtel, and R. Kessler. 2013. Survey shows that fewer than a third of patient-centered medical home practices engage patients in quality improvement. Health Affairs 2:368-375. https://doi.org/10.1377/hlthaff.2012.1183
- Hannemann-Weber, H., M. Kessel, K. Budych, and C. Schultz. 2011. Shared communication processes within healthcare teams for rare diseases and their influence on healthcare professionals’ innovative behavior and patient satisfaction. Implementation Science 6:40. https://doi.org/10.1186/1748-5908-6-40
- Harrington, K. 2012. The use of metaphor in discourse about cancer: A review of the literature. Clinical Journal of Oncology Nursing 16(4):408-412. https://doi.org/10.1188/12.CJON.408-412
- Haskard, K., S. Williams, M. DiMatteo, R. Rosenthal, M. White, and M. Goldstein. 2008. Physician and patient communication training in primary care: Effects on participation and satisfaction. Health Psychology 27(5):513-522. https://doi.org/10.1037/0278-6133.27.5.513
- Havyer, R., M. Wingo, N. Comfere, D. Nelson, A. Halvorsen, F. McDonald, and D. Reed. 2014. Teamwork assessment in internal medicine: A systematic review of validity evidence and outcomes. Journal of General Internal Medicine 29(6):894-910. https://doi.org/10.1007/s11606-013-2686-8
- Heyland, D., D. Barwich, D. Pichora, P. Dodek, F. Lamontagne, J. You, C. Tayler, P. Porterfield, T. Sinuff, J. Simon, and ACCEPT (Advance Care Planning Evaluation in Elderly Patients) Study Team; Canadian Researchers at the End of Life Network (CARENET). 2013. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Internal Medicine 173(9):778-787. https://doi.org/10.1001/jamainternmed.2013.180
- Hibbard, J., and H. Gilburt. 2014. Supporting people to manage their health: An introduction to patient activation. London, U.K.: The King’s Fund.
- Hibbard, J., E. Mahoney, R. Stock, and M. Tusler. 2007. Do increases in patient activation result in improved self- management behavior. Health Services Research Journal 42(4):1443-1463. https://doi.org/10.1111/j.1475-6773.2006.00669.x
- Hibbard, J., J. Greene, and M. Tusler. 2009. Improving the outcomes of disease management by tailoring care to the patient’s level of activation. American Journal of Managed Care 15(6):353-360. Available at: https://pubmed.ncbi.nlm.nih.gov/19514801/ (accessed June 24, 2020).
- Hibbard, J., J. Greene, and V. Overton. 2013. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores.’ Health Affairs vol. 32(2):216-222. https://doi.org/10.1377/hlthaff.2012.1064
- Hoegl, M., and H. Gemuenden. 2001. Teamwork quality and the success of innovative projects: A theoretical concept and empirical evidence. Organization Science 12:435-449. https://doi.org/10.1287/orsc.12.4.435.10635
- Hudson, J., P. Knight, and K. Weston. 2012. Patient perceptions of innovative longitudinal integrated clerkships based in regional, rural and remote primary care: A qualitative study. BMC Family Practice 13:72. https://doi.org/10.1186/1471-2296-13-72
- Hynes, P., P. Conlon, J. O’Neill, and S. Lapinsky. 2008. Partners in critical care. Dynamics 19(1):12-17.
- IHI (Institute for Healthcare Improvement). 2014. The IHI Triple Aim. Available at: http://www.ihi.org/Engage/Initiatives/ TripleAim/Pages/default.aspx (accessed April 15, 2014).
- Institute of Medicine. 2001. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Academies Press. https://doi.org/10.17226/10027
- Jahng, K., L. Martin, C. Golin, and M. DiMatteo. 2005. Preferences for medical collaboration: Patient-physician congruence and patient outcomes. Patient Education and Counseling 57(3):308-314. https://doi.org/10.1016/j.pec.2004.08.006
- James, J. 2013. Health policy brief: Patient engagement. Health Affairs. Available at: https://www.healthaffairs.org/healthpolicybriefs/brief.php?brief_id=86 (accessed April 29, 2014).
- John A. Hartford Foundation. 2014. Public poll: On your team: What older adults think about team care and medical home services. Available at: http://www.jhartfound.org/learning-center/public-poll-on-your-team-howolder-adults-view-team-care-and-the-medical-home/ (accessed April 8, 2014).
- Kaplan, S., S. Greenfield, and J. Ware Jr. 1989. Assessing the effects of physician-patient interactions on the outcomes of chronic disease. Medical Care 27(3 Suppl):S110-S127. https://doi.org/10.1097/00005650-198903001-00010
- Kaplan, S., B. Gandek, S. Greenfield, W. Rogers, and J. Ware. 1995. Patient and visit characteristics related to physicians’ participatory decision-making style. Results from the Medical Outcomes Study. Medical Care 33(12):1176-1187. https://doi.org/10.1097/00005650-199512000-00002
- Klabunde, C., D. Lanier, E. Breslau, J. Zapka, R. Fletcher, D. Ransohoff, and S. Winawer. 2007. Improving colorectal cancer screening in primary care practice: Innovative strategies and future directions. Journal of General Internal Medicine 22(8):1195-1205. https://doi.org/10.1007/s11606-007-0231-3
- Knight, J. 2007. Change management in cancer care: A one-stop gynaecology clinic. British Journal of Nursing 16(18):1122-1126. https://doi.org/10.12968/bjon.2007.16.18.27505
- Knops, K., M. Srinivasan, and F. Meyers. 2005. Patient desires: A model for assessment of patient preferences for care of severe or terminal illness. Palliative & Supportive Care 3(4):289-299. https://doi.org/10.1017/s1478951505050455
- Körner, M., H. Ehrhardt, and A. Steger. 2013. Designing an interprofessional training program for shared decision making. Journal of Interprofessional Care 66(6):146-154. https://doi.org/10.3109/13561820.2012.711786
- Krikorian, S., and J. Fowler. 2008. A view from Riggs: Treatment resistance and patient authority—7. A team approach to treatment resistance. Journal of the American Academy of Psychoanalysis & Dynamic Psychiatry 36(2):353-373. https://doi.org/10.1521/jaap.2008.36.2.353
- Lane-Carlson, M., and J. Kumar. 2012. Engaging patients in managing their health care: Patient perceptions of the effect of a total joint replacement presurgical class. The Permanente Journal 16(3):42-47. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3442761/ (accessed June 24, 2020).
- Langford, A., D. Sawyer, S. Gioimo, C. Brownson, and M. O’Toole. 2007. Patient-centered goal setting as a tool to improve diabetes self-management. The Diabetes Educator 33(Suppl 6):139S-144S. https://doi.org/10.1177/0145721707304475
- Latta, L., R. Dick, C. Parry, and G. Tamura. 2008. Parental responses to involvement in rounds on a pediatric inpatient unit at a teaching hospital: A qualitative study. Academic Medicine 83(3):292-297. https://doi.org/10.1097/ACM.0b013e3181637e21
- Lee, P. 2007. What does partnership in care mean for children’s nurses? Journal of Clinical Nursing 16(3): 518-526. https://doi.org/10.1111/j.1365-2702.2006.01832.x
- Lemieux-Charles, L., and W. McGuire. 2006. What do we know about health care team effectiveness? A review of the literature. Medical Care Research and Review 63:263-300. https://doi.org/10.1177/1077558706287003
- Levack, W., S. Dean, R. Siegert, and K. McPherson. 2011. Navigating patient-centered goal setting in inpatient stroke rehabilitation: How clinicians control the process to meet perceived professional responsibilities. Patient Education and Counseling 85(2):206-213. https://doi.org/10.1016/j.pec.2011.01.011
- Lewis, P., and M. Tully. 2011. The discomfort caused by patient pressure on the prescribing decisions of hospital prescribers. Research in Social and Administrative Pharmacy 7(1):4-15. https://doi.org/10.1016/j.sapharm.2010.02.002
- Lindberg, E., U. Hörberg, E. Persson, and M. Ekebergh. 2013. It made me feel human—A phenomenological study of older patients’ experiences of participating in a team meeting. International Journal of Qualitative Studies on Health and Well-being (8). https://doi.org/10.3402/qhw.v8i0.20714
- Liptak, G., and N. Murphy. 2011. Providing a primary care medical home for children and youth with cerebral palsy. Pediatrics 128(5):e1321-e1329. https://doi.org/10.1542/peds.2011-1468
- Lown, B., J. Kryworuchko, C. Bieber, D. Lillie, C. Kelly, B. Berger, and A. Loh. 2011. Continuing professional development for interprofessional teams supporting patients in healthcare decision making. Journal of
Interprofessional Care 25(6):401-408. https://doi.org/10.3109/13561820.2011.583563 - Lubetkin, E., W. Lu, and M. Gold. 2010. Levels and correlates of patient activation in health center settings: Building strategies for improving health outcomes. Journal of health care for the poor and underserved 21(3):796-808. https://doi.org/10.1353/hpu.0.0350
- Mahon, M. 2010. Advanced care decision making: Asking the right people the right questions. Journal of Psychosocial Nursing and Mental Health Services 48(7):13-19. https://doi.org/10.3928/02793695-20100528-01
- Markova, T., M. Mateo, and L. Roth. 2012. Implementing teams in a patient-centered medical home residency practice: Lessons learned. Journal of the American Board of Family Medicine 25(2):224-231. https://doi.org/10.3122/jabfm.2012.02.110181
- Mathews, D. 1984. Dr. Marjory Warren and the origins of British Geriatrics. Journal of the American Geriatrics Society 32(4):253-258. https://doi.org/10.1111/j.1532-5415.1984.tb02017.x
- Mathieu, J., T. Maynard, T. Rapp, and L. Gilson. 2008. Team effectiveness 1997-2007: A review of recent advancements and a glimpse into the future. Journal of Management 34:410-476. https://doi.org/10.1177/0149206308316061
- Matthews, R., S. Wilson, J. Valentine, and J. Nota. 2010. Involving patients in service improvement. Nursing Management 16(10):16-19.
- McAllister, J., W. Cooley, J. Van Cleave, A. Boudreau, and K. Kuhlthau. 2013. Medical home transformation in pediatric primary care—what drives change? Annals of Family Medicine 11(Suppl 1):S90-S98. https://doi.org/10.1370/afm.1528
- McCauley, K., and R. Irwin. 2006. Changing the work environment in ICUs to achieve patient-focused care: The time has come. Chest 130(5):1571-1578. https://doi.org/10.1378/chest.130.5.1571
- McDaniel Jr., R., H. Jordan Lanham, and R. Anderson. 2009. Implications of complex adaptive systems theory for the design of research on health care organizations. Health Care Management Review 34(2): 191-199. https://doi.org/10.1097/HMR.0b013e31819c8b38
- McDonald, C., and A. McCallin. 2010. Interprofessional collaboration in palliative nursing: What is the patient-family role? International Journal of Palliative Nursing 16(6):286-289. https://doi.org/10.12968/ijpn.2010.16.6.48832
- Meltzer, L., E. Steinmiller, S. Simms, M. Grossman, Complex Care Consultation Team, and Y. Li. 2009. Staff engagement during complex pediatric medical care: The role of patient, family, and treatment variables. Patient Education and Counseling 74(1):77-83. https://doi.org/10.1016/j.pec.2008.07.051
- Mercer, L., P. Tanabe, P. Pang, M. Gisondi, D. Courtney, K. Engel, S. Donlan, J. Adams, and G. Makoul. 2008. Patient perspectives on communication with the medical team: Pilot study using the Communication Assessment Tool-Team (CAT-T). Patient Education and Counseling 73(2):220-223. https://doi.org/10.1016/j.pec.2008.07.003
- Miller, A., M. Weinger, P. Buerhaus, and M. Dietrich. 2010. Care coordination in intensive care units: Communicating across information spaces. Human Factors 52(2):147-161. https://doi.org/10.1177/0018720810369149
- Milman, U., S. Ben-Moshe, and D. Hermoni. 2005. The role of the patient care team in elderly people decision on influenza vaccination. Patient Education and Counseling 58(2):203-208. https://doi.org/10.1016/j.pec.2004.08.017
- Mitchell, P., M. Wynia, R. Golden, B. McNellis, S. Okun, C.E. Webb, V. Rohrbach, and I. Von Kohorn. 2012. Core principles & values of effective team-based health care. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201210c
- Mosen, D., J. Schmittdiel, J. Hibbard, D. Sobel, C. Remmers, and J. Bellows. 2007. Is patient activation associated with outcomes of care for adults with chronic conditions? The Journal of Ambulatory Care Management 30(1):21-9. https://doi.org/10.1097/00004479-200701000-00005
- Murphy, N., and P. Carbone. 2011. Parent–provider–community partnerships: Optimizing outcomes for children with disabilities. Pediatrics 128(4):795-802. https://doi.org/10.1542/peds.2011-1467
- Nagel, K., L. Wizowski, J. Duckworth, J. Cassano, S. Hahn, and M. Neal. 2008. Using plain language skills to create an educational brochure about sperm banking for adolescent and young adult males with cancer.
Journal of Pediatric Oncology Nursing 25(4):220-226. https://doi.org/10.1177/1043454208319973 - National Patient Safety Foundation. 2011. The universal patient compact: Principles for partnership. Available at: http://www.npsf.org/wp-content/uploads/2011/10/UniversalPatientCompact.pdf (accessed March 14, 2014).
- NCQA (National Committee for Quality Assurance). 2014. The future of patient-centered medical homes: Foundation for a better health care system. Available at: http://www.ncqa.org/Portals/0/Public%20Policy/2014%20
Comment%20Letters/The_Future_of_PCMH.pdf (accessed April 17, 2014). - Oandasan, I., L. Conn, L. Lingard, A. Karim, D. Jakubovicz, C. Whitehead, K. L. Miller, N. Kennie, and S. Reeves. 2009. The impact of space and time on interprofessional teamwork in Canadian primary health care settings: Implications for health care reform. Primary Health Care Research and Development 10(2):151-162. https://doi.org/10.1017/S1463423609001091
- O’Connell, J. 2012. Management of obesity: Lessons learned from a multidisciplinary team. European Diabetes Nursing 9(1):26-29. https://doi.org/10.1002/edn.200
- Orchard, C., V. Curran, and S. Kabene. 2005. Creating a culture for interdisciplinary collaborative professional practice. Medical Education Online 10:1-13. https://doi.org/10.3402/meo.v10i.4387
- Parker Oliver, D., D. Porock, G. Demiris, and K. Courtney. 2005. Patient and family involvement in hospice interdisciplinary teams. Journal of Palliative Care 21(4):270-276. Available at: https://pubmed.ncbi.nlm.nih.gov/16483096/ (accessed June 24, 2020).
- Parker Oliver, D., G. Demiris, E. Wittenberg-Lyles, and D. Porock. 2010a. The use of videophones for patient and family participation in hospice interdisciplinary team meetings: A promising approach. European Journal of Cancer Care 19(6):729-735. https://doi.org/10.1111/j.1365-2354.2009.01142.x
- Parker Oliver, D., G. Demiris, E. Wittenberg-Lyles, D. Porock, J. Collier, and A. Arthur. 2010b. Caregiver participation in hospice interdisciplinary team meetings via videophone technology: A pilot study to improve pain management. American Journal of Hospice & Palliative Medicine 27(7):465-473. https://doi.org/10.1177/1049909110362402
- Peek, M., A. Odoms-Young, M. Quinn, R. Gorawara-Bhat, S. Wilson, and M. Chin. 2010. Race and shared decision-making: Perspectives of African-Americans with diabetes. Social Science & Medicine 71(1):1-9. https://doi.org/10.1016/j.socscimed.2010.03.014
- Post, D., D. Cegala, and W. Miser. 2002. The other half of the whole: Teaching patients to communicate with physicians. Family Medicine 34(5):344-352. Available at: https://www.ncbi.nlm.nih.gov/books/NBK69300/ (accessed June 24, 2020).
- Pritchard Kennedy, A. 2012. Systematic ethnography of school-age children with bleeding disorders and other chronic illnesses: Exploring children’s perceptions of partnership roles in family-centered care of their chronic illness. Child: Care, Health and Development 38(6):863-869. https://doi.org/10.1111/j.1365-2214.2011.01310.x
- Ronan, J. 2013. Tailored care management with patient-centered web-based portal in primary health care: Sustaining a relational context. Studies in Health Technology and Informatics 183:319-324. Available at: https://pubmed.ncbi.nlm.nih.gov/23388306/ (accessed June 24, 2020).
- Rosen, P., E. Stenger, M. Bochkoris, M. Hannon, and C. Kwoh. 2009. Family-centered multidisciplinary rounds enhance the team approach in pediatrics. Pediatrics 123(4):e603-e608. https://doi.org/10.1542/peds.2008-2238
- Rosher, R., and S. Robinson. 2005. Impact of the Eden Alternative on family satisfaction. American Medical Directors Association 6(3):189-193. https://doi.org/10.1016/j.jamda.2005.03.005
- Rushton, C. 2007. Respect in critical care: A foundational ethical principle. AACN Advanced Critical Care 18(2):149-156. https://doi.org/10.1097/01.AACN.0000269258.14418.1e
- Rusk, H. 1972. A world to care for: The autobiography of Howard A. Rusk. New York: Random House.
- RWJF (Robert Wood Johnson Foundation). 2014. Compendium: Tools for engaging patients in your practice. Available at: http://forces4quality.org/compendium-tools-engaging-patients-your-practice (accessed September 18, 2014).
- Salas, E., T. Dickinson, S. Converse, and S. Tannenbaum. 1992. Toward an understanding of team performance and training. Teams: Their training and performance. Norwood, NJ: Ablex. Pp. 3-29.
- Sequist, T., T. von Glahn, A. Li, W. Rogers, and D. Safran. 2009. Statewide evaluation of measuring physician delivery of self-management support in chronic disease care. Journal of General Internal Medicine 24(8):939-945. https://doi.org/10.1007/s11606-009-1033-6
- Serrano-Gil, M., and S. Jacob. 2010. Engaging and empowering patients to manage their type 2 diabetes, Part I: A knowledge, attitude, and practice gap? Advances in Therapy 27(6):321-333. https://doi.org/10.1007/s12325-010-0071-0
- Shively, M., N. Gardetto, M. Kodiath, A. Kelly, T. Smith, C. Stepnowsky, C. Maynard, and C. Larson. 2013. Effect of patient activation on self-management in patients with heart failure. The Journal of cardiovascular nursing 28(1):20-34. https://doi.org/10.1097/JCN.0b013e318239f9f9
- Shoemaker, S., J. Schaefer, M. Parchman, K. Fuda, J. Levin, M. Hunt, and R. Ricciardi. 2013 (unpublished). Agency for Healthcare Research and Quality.
- Sisterhen, L., R. Blaszak, M. Woods, and C. Smith. 2007. Defining family-centered rounds. Teaching and Learning in Medicine 19(3):319-322. https://doi.org/10.1080/10401330701366812
- Smith, Q., R. Street Jr., R.Volk, and M. Fordis. 2013. Differing levels of clinical evidence: Exploring communication challenges in shared decision making. Medical Care Research and Review 70(1 Suppl):3S-13S. https://doi.org/10.1177/1077558712468491
- Smits, S., D. Bowden, J. Falconer, and D. Strasser. 2014. Improving medical leadership and teamwork: An iterative process. Leadership in Health Services 27(4):299-315. https://doi.org/10.1108/LHS-02-2014-0010
- Sommers, R., S. Goold, P. McGlynn, and M. Danis. 2013. Focus groups highlight that many patients object to clinicians’ focusing on cost. Health Affairs 32:338-346. https://doi.org/10.1377/hlthaff.2012.0686
- Stevens, A., D. Strasser, J. Uomoto, S. Bowen, and J. Falconer. 2007. Utility of treatment implementation methods in a clinical trial with rehabilitation teams. Journal of Rehabilitation Research & Development 44(4):537-546. https://doi.org/10.1682/JRRD.2006.09.0120
- Strasser, D., and J. Falconer. 1997. Linking treatment to outcomes: Building a conceptual model of rehabilitation team. Topics in Stroke Rehabilitation 4(1):15-17. https://doi.org/10.1310/KL5R-U470-VF9M-3HLN
- Strasser, D., J. Falconer, A. Stevens, J. Uomoto, J. Herrin, S. Bowen, and A. Burridge. 2008. Team training and stroke rehabilitation outcomes: A cluster randomized trial. Archives of Physical Medicine and Rehabilitation 89:10-15. https://doi.org/10.1016/j.apmr.2007.08.127
- Street Jr., R., H. Gordon, M. Ward, E. Krupat, and R. Kravitz. 2005. Patient participation in medical consultations: Why some patients are more involved than others. Medical Care 43(10):960-969. https://doi.org/10.1097/01.mlr.0000178172.40344.70
- Taplin, S., M. Foster, and S. Shortell. 2013. Organizational leadership for building effective health care teams. Annals of Family Medicine 11(3):279-280. https://doi.org/10.1370/afm.1506
- Toles, M., J. Barroso, C. Colón-Emeric, K. Corazzini, E. McConnell, and R. Anderson. 2012. Staff interaction strategies that optimize delivery of transitional care in a skilled nursing facility: A multiple case study. Family & Community Health 35(4):334-344. https://doi.org/10.1097/FCH.0b013e31826666eb
- Ueno, N., T. Ito, R. Grigsby, M. Black, and J. Apted. 2010. ABC conceptual model of effective multidisciplinary cancer care. Nature Reviews Clinical Oncology 7(9):544-547. https:/.doi.org/10.1038/nrclinonc.2010.115
- van der Eijk, M., M. Faber, J. Aarts, J. Kremer, M. Munneke, and B. Bloem. 2013. Using online health communities to deliver patient-centered care to people with chronic conditions. Journal of Medical Internet Research 15(6):e115. https://doi.org/10.2196/jmir.2476
- Van Norman, G. 1998. Interdisciplinary team issues. Seattle, WA: University of Washington School of Medicine. Available at: http://depts.washington.edu/bioethx/topics/team.html (accessed June 24, 2013).
- Virtual Mentor. 2013. Physician leadership and team-based care. Available at: http://virtualmentor.ama-assn.org/2013/06/ toc-1306.html (accessed October 2, 2014).
- Watt, L., D. Dix, S. Gulati, L. Sung, R. Klaassen, N. Shaw, and A. Klassen. 2013. Family-centred care: A qualitative study of Chinese and South Asian immigrant parents’ experiences of care in paediatric oncology. Child: Care, Health and Development 39(2):185-193. https://doi.org/10.1111/j.1365-2214.2011.01342.x
- Weingart, S., J. Zhu, L. Chiappetta, S. Stuver, E. Schneider, A. Epstein, J. David-Kasdan, C. Annas, J. Fowler, and J. Weissman. 2011. Hospitalized patients’ participation and its impact on quality of care and patient safety. International Journal for Quality in Health Care 23(3):269-277. https://doi.org/10.1093/intqhc/mzr002
- White, D., S. Cua, R. Walk, L. Pollice, L. Weissfeld, S. Hong, C. Landefeld, and R. Arnold. 2012. Nurse-led intervention to improve surrogate decision making for patients with advanced critical illness. American Journal of Critical Care 21(6):396-409. https://doi.org/10.4037/ajcc2012223
- Wittenberg-Lyles, E. 2005. Information sharing in interdisciplinary team meetings: An evaluation of hospice goals. Qualitative Health Research 15(10):1377-1391. https://doi.org/10.1177/1049732305282857
- Wittenberg-Lyles, E., D. Parker Oliver, G. Demiris, P. Baldwin, and K. Regehr. 2008a. Communication dynamics in hospice teams: Understanding the role of chaplain in interdisciplinary team collaboration. Journal of Palliative Medicine 11(10):1330-1335. https://doi.org/10.1089/jpm.2008.0165
- Wittenberg-Lyles, E., D. Parker Oliver, G. Demiris, B. Petty, and M. Day. 2008b. Caregiver involvement in hospice interdisciplinary team meetings: A case study. Journal of Palliative Care 24(4):277-279. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2675180/ (accessed June 24, 2020).
- Wittenberg-Lyles, E., D. Parker Oliver, G. Demiris, and P. Baldwin. 2010a. The ACTive intervention in hospice interdisciplinary team meetings: Exploring family caregiver and hospice team communication. Journal of Computer-Mediated Communication 15(3):465-481. https://doi.org/10.1111/j.1083-6101.2010.01502.x
- Wittenberg-Lyles, E., D. Parker Oliver, G. Demiris, S. Burt, and K. Regehr. 2010b. Inviting the absent members: Examining how caregivers’ participation affects hospice team communication. Palliative Medicine 24(2):192-195. https://doi.org/10.1177/0269216309352066
- Wittenberg-Lyles, E., D. Parker Oliver, G. Demiris, A. Rankin, S. Shaunfield, and R. Kruse. 2012. Conveying empathy to hospice family caregivers: Team responses to caregiver empathic communication. Patient Education and Counseling 89(1):31-37. https://doi.org/10.1016/j.pec.2012.04.004
- Wittenberg-Lyles, E., D. Parker Oliver, R. Kruse, G. Demiris, L. Gage, and K. Wagner. 2013. Family caregiver participation in hospice interdisciplinary team meetings: How does it affect the nature and content of communication? Health Communication 28(2):110-118. https://doi.org/10.1080/10410236.2011.652935
- Wood, D., Q. McCaskill, N. Winterbauer, E. Jobli, T. Hou, P. Wludyka, K. Stowers, and W. Livingood. 2009. A multi-method assessment of satisfaction with services in the medical home by parents of children and youth with special health care needs (CYSHCN). Maternal and Child Health Journal 13(1):5-17. https://doi.org/10.1007/s10995-008-0321-9
- Wottrich, A., L. von Koch, and K. Tham. 2007. The meaning of rehabilitation in the home environment after acute stroke from the perspective of a multi-professional team. Physical Therapy 87(6):778-788. https://doi.org/10.2522/ptj.20060152
- Wynia, M., I. Von Kohorn, and P. Mitchell. 2012. Challenges at the intersection of team-based and patient-centered health care. Insights from an IOM working group. JAMA 308(13):1327-1328. https://doi.org/10.1001/jama.2012.12601
- Wynia, M., P. Mitchell, S. Okun, C. E. Webb, R. McNellis, R. Golden, V. Rohrbach, and I. Von Kohorn. Patient roles on health care teams reflect communication and decision-making models. 2013 (unpublished).
- Xyrichis, A., and E. Ream 2008. Teamwork: A concept analysis. Journal of Advanced Nursing 61(2):232-241. https://doi.org/10.1111/j.1365-2648.2007.04496.x